In late June, Jazz Pharmaceuticals began to market a drug aimed at treating people whose metastatic small cell lung cancer has not responded to an initial round of chemotherapy.
The drug, lurbinectedin, was developed by Madrid-based PharmaMar S.A., which in December 2019 signed a licensing agreement with Jazz. This permitted Jazz to sell the drug in the United States under the brand name Zepzelca. (Lurbinectedin had failed a clinical trial for ovarian cancer in 2018.) Dublin-based Jazz, with its shares listed on the Nasdaq, has significant U.S. operations in Philadelphia and Palo Alto, California.
For U.S. oncologists who treat individuals with small cell lung cancer, lurbinectedin’s arrival was a big deal. Dr. H. Jack West recalled his cautious optimism upon reading of lurbinectedin’s initial clinical trial results last June, especially since few therapies existed for people with small cell lung cancer.
An associate clinical professor in medical oncology at City of Hope’s department of medical oncology and therapeutics research in Duarte, California, West told the Foundation for Financial Journalism that lurbinectedin’s “results in Phase II were [notable] because it was a decent-sized trial [of 105 people] and the drug seemed to have a measurable effect on a subset of patients.”
The meager number of small cell cancer drugs in the development pipeline has led some oncologists to desperately embrace any treatment showing even modest promise, said West, who added that he has seen doctors “cheerleading” for pharmaceutical companies with products in trials and forgoing skepticism about existing treatments.
Despite the fact that Zepzelca was on the market for only six months of last year, it generated 4 percent of Jazz’s 2020 revenue, or $90.4 million. Jazz’s investors apparently loved the earnings boost from lurbinectedin sales; the company’s market capitalization climbed by more than $1.7 billion.
But the Food and Drug Administration has permitted lurbinectedin’s sale in the United States only under its accelerated approval program. The FDA required that PharmaMar conduct a confirmatory trial to prove the drug’s clinical benefit before seeking full approval.
PharmaMar had initially proposed in December 2018 that Phase III of lurbinectedin’s clinical trial serve as its confirmatory trial; the FDA granted this request in June 2020. (The FDA requests confirmatory trials only for accelerated approval program drugs.)
Yet by Dec. 3, Jazz and PharmaMar disclosed that lurbinectedin had failed to meet the primary endpoint of its clinical trial’s Phase III: achieving improvement in the overall survival of participants. The medication did not succeed in proving its benefit to study participants over the standard of care offered by already approved treatments for small cell lung cancer.
The FDA, however, did not pull the drug off the market. This lack of a response is becoming commonplace: The agency has permitted many drugs in the accelerated approval program to remain commercially available after their Phase III clinical trial failures.
Tackling daunting hurdles
While many cancers are lethal, and cancer treatments are generally complex and expensive, small cell lung cancer poses a special challenge.
Named after the cancer cell’s size and shape when viewed through a microscope, small cell lung cancer will cause about 13 percent of the 235,760 newly diagnosed cases of lung cancer in the United States this year, the American Society of Clinical Oncology has projected. Compared with the wealth of information known about other cancers, relatively little is understood about how small cell lung cancer metastasizes. The tumors typically develop in air passages around the windpipe — especially in older smokers — and rapidly spread to other organs. This happens so quickly that almost 70 percent of individuals with the disease have experienced metastasis by the time of their first diagnosis. Chemotherapy might later appear to have eradicated tumors, only to have them grow back.
Just 6 percent of people diagnosed with metastatic small cell lung cancer live five more years, according to the American Society of Clinical Oncology. In comparison, 13 percent of people diagnosed with metastatic pancreatic cancer reach that milestone.
Pharmaceutical companies such as AbbVie, Poniard Pharmaceuticals and United Therapeutics have poured billions of dollars into the development of drugs for small cell lung cancer and clinical trials, but few life-extending options have materialized over the past three decades. All told, 40 clinical trials for small cell lung cancer treatments have failed.
Failing scientifically, yet scoring commercially
Traditionally, the FDA has viewed a drug’s inability to outperform current treatments in extending or improving the life of study participants as disqualifying — except for medications in its accelerated approval program, such as lurbinectedin. And lurbinectedin, like many cancer drugs, has documented side effects including fatigue, nausea and declines in white blood cell counts.
Commercially, though, lurbinectedin has been far from a failure, and brokerage analysts have projected that Jazz could take in $200 million to $225 million in revenue this year from sales of the drug. One Wells Fargo analyst, in a June 2020 research note went so far as to suggest that Zepzelca’s annual sales might peak at $700 million. PharmaMar is benefitting handsomely, too: Jazz’s annual report noted the $300 million in payments it made to PharmaMar last year.
And the actions of Jazz stand in sharp contrast with those of larger rivals with oncology drugs. After Bristol Myers Squibb and Merck recently disclosed the failure of confirmatory trials for their own bestselling drugs under accelerated FDA approval for treatment of small cell lung cancer, both companies immediately stopped marketing them for that purpose and removed the indication from their labels. Bristol Myers Squibb’s Opdivo and Merck’s Keytruda are still indicated for the treatment of other cancers, including non-small cell lung cancer, though.
The FDA is rather vague about what is supposed to happen after a drug in the accelerated approval program fails its confirmatory trial. The FDA’s website simply states that the agency has “procedures in place that could lead to removing the drug from market.”
FDA press officer Chanapa Tantibanchachai wrote in an email reply to the Foundation for Financial Journalism’s questions, “The FDA is committed to ensuring the integrity of the accelerated approval program. The agency is currently in the process of evaluating oncology accelerated approvals.”
(On April 27, the FDA’s Oncologic Drugs Advisory Committee will hold a public hearing to examine accelerated approval drugs “with confirmatory trials that have not verified clinical benefits,” the agency has announced.)
Over the past two decades, the FDA appears to have shifted away from evaluating a drug solely on its trial data in favor of also including other data sets, according to Dr. Thomas Frieden, a former director of the Centers for Disease Control and Prevention. Thus, U.S. regulators might not remove medications like lurbinectedin from the marketplace in the near future.
At the center of this shifting regulatory landscape is the FDA’s acting leader, Dr. Janet Woodcock, who has served two long stints at the helm of the agency’s Center for Drug Evaluation and Research. Dr. Woodcock has been a vocal advocate of accommodating the pharmaceutical industry to speed the availability of drugs. She is well-known for regulatory leniency toward drugs whose clinical trials cast doubts on their efficacy.
What is less clear is how people with small cell lung cancer would benefit from access to expensive drugs that rarely work well, if at all.
Sacrificing clinical rigor, a casualty of war on cancer
The nature of cancer, and particularly small cell lung cancer, results in very complex and brutal tradeoffs as researchers and pharmaceutical companies hasten to bring new drugs to market.
While the randomized controlled trial has been long accepted as the best way to determine whether a drug is effective and safe for the largest possible population, this method poses problems for small cell lung cancer studies.
A clinical trial’s Phase III — which can take as long as four years to assess a drug’s safety and efficacy against the current standard of care — would appear unwieldy if a disease is causing more than 90 percent of the afflicted individuals to die before five years have elapsed.
One technique developed by clinical researchers is using surrogate endpoints, or substitute evaluation criteria. Researchers believe these data points might correlate with two traditional clinical endpoints: extending life or improving its quality.
For example, the data that initially caught Dr. West’s eye in Phase II of lurbinectedin’s clinical trial was a surrogate endpoint called the overall response rate. (The FDA has at times called it an objective response rate.) This can involve measuring a tumor’s size over a period of weeks as a someone takes a drug. (In lurbinectedin’s case, 35 percent of the study participants, or 37 individuals, had their tumors shrink 30 percent or more, with the effect lasting on average slightly less than five months.)
Another popular surrogate measurement for cancer trials is progression-free survival. This is calculated from the time after tumors stop growing (or disappear) until they grow again.
While progression-free survival and tumor shrinkage are certainly welcome developments, for people with small cell lung cancer they are often temporary events, given how common it is for tumors to grow back.
What’s more, a 2018 report in Clinical Cancer Research found that overall response rate and progression-free survival are poor predictors of a person’s overall survival.
A more detailed analysis of the tenuous links between response rate and increased patient life appeared in a Journal of the American Medical Association article in May 2019 by three doctors at Oregon Health & Science University: Emerson Chen, Vikram Raghunathan and Vinay Prasad. They examined 85 indications for 59 oncology drugs that were granted FDA approval based on response rate and found that only six of them extended life span. (Some of these drugs were in the accelerated approval program; others were not.)
The FDA does not seem to have taken this research into account, however. In June 2018, FDA researchers published a triumphant review of the accelerated approval program’s first 25 years. From 1992 to 2018, the agency approved 93 indications for 64 products through the program, with only five indications subsequently withdrawn.
But to Harvard Medical School’s Dr. Aaron Kesselheim, the FDA is evaluating its accelerated approval program backward. In a May 2019 JAMA article that made a big splash, Dr. Kesselheim and two colleagues, Drs. Bishal Gyawali and Spencer Phillips Hey, examined the 93 drug indications allowed through the FDA’s accelerated approval program. “We looked ‘underneath the hood’ at the FDA’s basis for approving those [93 indications of] drugs,” said Dr. Kesselheim during a Foundation for Financial Journalism interview. “Our question was simple: ‘Is there evidence that using [the FDA’s accelerated approval] pathway provides drugs that benefit patients?’”
Their answer: not really. Only 19 of the 93 indications investigated by Dr. Kesselheim and his colleagues, or slightly more than 20 percent, demonstrated any improvement in overall survival during Phase III of their clinical trials.
The real problem with the program, said Dr. Kesselheim, lies with the FDA’s use of “surrogate measures that are not clinically validated” for evaluating drugs. “There are valid uses for surrogate endpoints” in clinical trials, he noted: A drug’s effect can be measured faster by using a surrogate endpoint in lieu of a traditional clinical endpoint (which could require two years of study or more.)
“But with no clinical validation, surrogate measures can waste a lot of time,” Dr. Kesselheim added.
Setting standards, while benefitting financially
Another factor in lurbinectedin’s success thus far is tied to the role of the nonprofit National Comprehensive Cancer Network. While most Americans might be unaware of this organization, its work has possibly touched them in some way. As an alliance of 31 cancer treatment hospitals, the network has stated its mission is to develop “evidence-based guidelines” for the screening and treatment of 59 different types of cancer.
Although adoption of the network’s guidelines is voluntary, health care providers broadly accept its opinions for setting the standard of care for these cancer types. The network’s appeal lies in the fact that its 60 panels of experts include not only experienced oncologists but also pharmacists, research scientists and nurses. The panels investigate the minutiae of treatment details and even make their own assessments of various medicines and dosage levels.
Nonetheless, what health care professionals may not clearly see is how responsive to corporate interests the network’s small cell lung cancer panel has been.
On April 29, Francois Di Trapani, Jazz’s vice president for global scientific affairs, wrote the National Comprehensive Cancer Network’s small cell lung cancer panel to request that its clinical guidelines include lurbinectedin as a treatment option. He then followed up on June 15 to alert the panel to lurbinectedin’s selection for the accelerated access program.
By July 7, the nonprofit network’s small cell lung cancer panel had added lurbinectedin to its clinical practice guidelines.
Yet six doctors among the 30 physicians on this small cell lung cancer panel have disclosed that they have received payment from Jazz: five for serving as a Jazz scientific advisory board member, consultant or expert witness, and one other for participating as a Jazz promotional advisory board or speakers’ bureau member or consultant.
Because the Centers for Medicare and Medicaid Services will not update its Open Payments database of corporate payments to physicians to reflect 2020’s totals until sometime this June, the amounts are not yet publicly available.
One of the network’s six small cell lung cancer panelists who received a Jazz payment gave an enthusiastic November interview to a trade publication, touting lurbinectedin’s prospects: Dr. Apar Ganti, an oncologist and hematologist at the University of Nebraska Medical Center, declared to the American Journal of Managed Care that his panel had swiftly acted to recommend lurbinectedin’s use since few drugs are available to treat small cell lung cancer. His interview did not disclose his acceptance of money from Jazz, the very company marketing the drug in the States.
The Foundation for Financial Journalism reached out for comment to Dr. Ganti and the five other physician panelists paid by Jazz, Drs. Anne Chiang, Afshin Dowlati, Jonathan Goldman, Wade Iams and Jacob Sands but did not hear back.
Asked for comment, the network’s CEO, Dr. Robert Carlson, said the panel chose to recommend lurbinectedin’s use in its clinical guidelines based on a Lancet Oncology study published in May. Carlson added that the panel members make guideline updates “as supported by scientific evidence.” Nonetheless, the Lancet study was funded by PharmaMar and one of its authors, Dr. Sands, is among the six physician panelists who received money from Jazz.
Multiple attempts to obtain comment from Jazz’s management were unsuccessful.
If someone wanted to use a Venn diagram to illustrate what is wrong with the U.S. health care system, picking the different sets would be easy: Price gouging, abuse of loopholes, hidden risks to patients, baffling regulatory decisions, marginal efficacies and the use of doctor payments to stimulate drug sales would be some logical choices.
And a case in point would be Corcept Therapeutics, a specialty pharmaceutical company based in Menlo Park, California, and the apparent union of all things expensive and opaque. So how did Corcept, a small company with just one drug aimed at treating a tiny population of patients with a rare pituitary disorder, wind up there?
Corcept has managed to make handsome profits by quietly yet efficiently exploiting gaps in the nation’s health care regulatory framework. And its sole drug is none other than the storied mifepristone, better known as the abortion pill. While Roussel-Uclaf developed mifepristone in France in 1980, it became famous in the U.S. in 2000 when the Food and Drug Administration ruled that doctors could prescribe it to induce an abortion; it was sold as RU-486.
Just before that, two doctors at Stanford University Medical School’s psychiatry department began examining mifepristone for quite another use. In the mid-1990s Dr. Joseph Belanoff began testing a longstanding hypothesis of then-department chairman Dr. Alan Schatzberg that mifepristone could block the body’s production of cortisol and be used to help treat episodic psychosis, a condition that’s found in about 15 percent of people with major depressive disorder.
Encouraged by the results they observed in the few patients they tested, the doctors founded Corcept in 1998, with Stanford University’s technology licensing office serving as a silent third partner; the university had applied for a patent covering mifepristone’s use in treating depression.
But a preliminary study of mifepristone, released in the journal Biological Psychiatry in 2002, kicked off the academic equivalent of a food fight when several veteran psychiatric researchers argued that the test results provided no statistical backing for Schatzberg’s claims. One high-profile critic told the San Jose Mercury News in 2006 that the study was an “experimercial,” or an experiment whose purpose was to generate publicity rather than meaningful results.
These critics were onto something: In 2007 Corcept halted its clinical trial for the drug’s treatment of depression and did not publish the results, a development that usually means that the findings were not positive.
Faced with the prospect of the company’s business model collapsing, Corcept’s management managed to pull off what an April 2018 Kaiser Health News article called a “Hail Mary” when it sought — and received — Food and Drug Administration approval to test mifepristone as an orphan drug for the treatment of Cushing’s syndrome.
Endogenous Cushing’s syndrome is a pituitary gland disorder whereby the body is prompted to make too much adrenocorticotropic hormone, which governs the level of cortisol. And people with hypercortisolism — who overproduce cortisol — might have their metabolic functions go awry; this could lead to a host of painful and dangerous symptoms like rapid weight gain, skin discoloration, bone loss, heart disease and diabetes.
The primary culprit behind endogenous Cushing’s syndrome is a tumor that grows on the pituitary gland; in 70 percent to 90 percent of these cases, surgery to remove the tumor can successfully address the condition, according to the Pituitary Society.
But for as many as 30 percent or so of the people with Cushing’s syndrome (individuals who can’t undergo surgery or for whom surgery doesn’t mitigate these symptoms), Corcept developed a mifepristone treatment. And on Feb. 17, 2012, the FDA approved Corcept’s application to market its mifepristone medication Korlym as an orphan drug. The label, or the official designation for what it was approved to treat, is very specific: Korlym is to be prescribed only to people with endogenous Cushing’s syndrome who have both hypercortisolism and diabetes in order to reduce side effects of hyperglycemia, or high blood sugar levels.
The fact that the FDA had granted an approval allowing the company to market Korlym, however, doesn’t mean Corcept had scientifically demonstrated the drug’s success in treating Cushing’s syndrome.
Southern Investigative Reporting Foundation readers may recall from previous reporting on Acadia Pharmaceuticals that the FDA can sharply relax evidentiary standards when confronted with a small patient population possessing a rare disease.
Indeed, the FDA approved Korlym based on a single open-label study consisting of one group of 50 patients. (An open-label study is the least rigorous type of scientific investigation.) All participants in the study knew they were receiving the drug — and not a placebo — which risked the possible introduction of bias. And the study lacked a comparison group, whose results could be contrasted with those of the drug’s recipients. Plus, 36 of the 50 study participants reported protocol violations.
The FDA’s risk assessment and risk mitigation review for this study did conclude that Korlym’s trial design was flawed without the testing of an approved comparator drug, but “the progressive and serious nature of [Cushing’s syndrome] would make it unethical to randomize any patients to placebo.”
When the company tried to expand Korlym’s sales by seeking approval to market it in Europe, other problems emerged. In March 2015 Corcept withdrew its application for Corluxin (a renamed Korlym) after receiving a final round of questions from a committee of the European Medicines Agency and declining to answer them; the company cited “strategic business reasons” for ending the process.
In a late December 2018 interview, Corcept’s CFO Charles Robb told the Southern Investigative Reporting Foundation that the reason the company pulled Corluxin’s application was “primarily commercial.”
Robb said, “We just at the end of the day couldn’t figure how we would make any money [in Europe] selling it, given the way they priced [orphan] drugs.”
The European Medicines Agency had a starkly different view of events. In a brief “question and answers” release posted online in May 2015, the agency’s committee said its “provisional opinion” was against approving the drug. Three weeks later in a more formal assessment, it cited a laundry list of concerns, including the company’s failure to control the introduction of impurities during manufacturing, the design of the clinical trial and “limited” evidence of effectiveness.
Robb did not respond to a follow-up call and email with questions from the Southern Investigative Reporting Foundation about why Corcept spent the time and money to pursue approval of its drug all the way to the last stage of the process before realizing it couldn’t make money in Europe.
Asked about the recent sharp increase in the number of deaths recorded for Korlym in the FDA’s adverse events reporting system (FAERS), to 37 in the first nine months of 2018 from 17 for all of 2017, Robb was adamant that none of the deaths could be directly attributed to Korlym. In response to a question about how he could be certain of that, he said, “All [the FAERS death reports] are adjudicated by a third party”: Robb added that Corcept retains Ashfield to provide pharmacovigilance, a service that evaluates reports of a drug’s adverse events for a manufacturer. And he insisted that the medicine and its dosage were not responsible for any of 103 deaths reported for Korlym since 2012. He did not answer a question about why 17 of the 103 death reports mentioned “product used for unknown indication.”
A brief aside: Adverse event reports are a tabulation of patient responses to a drug. The reports are unverified and are not designed to replace a formal investigation or autopsy. This completely voluntary reporting system allows for a wide array of filers, and with family members, caregivers and trained medical professionals able to make submissions, the level of accuracy and detail varies widely. Finally, many medical professionals have suggested that because this documentation is voluntary, incidents involving newer drugs are not reported to FAERS.
(To present a more nuanced view of patient deaths on Korlym, the Southern Investigative Reporting Foundation obtained longer form FAERS reports via the Freedom of Information Act. While not official reports, they do provide valuable context and data, such as dosage, basic health datapoints, initial diagnosis and the duration of Korlym use. Accordingly, any instances where the circumstances of a patient’s death suggested that a reaction to Korlym was secondary were eliminated.)
Ashfield officials did not return a call seeking comment.
Robb did, however, have a lengthy list of possible causes for these deaths: “The thing to understand is these patients are very ill. Some of them have adrenal cancer,” he said, “Some of them ahead have been suffering from the symptoms of Cushing’s syndrome for decades; some are simply elderly and the list of medications these patients have to take can be 20 and 30 drugs long.”
————————
Nonetheless, as Corcept’s recent income statements show, the company has certainly figured out a way to make quite a bit of money in the United States from selling this drug. Corcept’s road to success in this country has followed the tried and true specialty pharmaceutical playbook, raising a medication’s price steeply and often, while using physician speakers bureau payments to build drug awareness.
The public battering of other specialty pharmaceutical company CEOs after they tried to defend price increases might have given Corcept’s Dr. Belanoff the idea of acknowledging unpleasant facts first — before others do. Thus in April 2018 Dr. Belanoff told Kaiser Health News, “We have an expensive drug, there’s no getting around that,” perhaps in an effort to diffuse some of the sticker shock of his drug’s price tag, which he later cited as $180,000.
But that’s not anywhere close to a person’s cost for a year’s worth of Korlym prescriptions. Dr. Belanoff’s quote is only for the annual price for prescriptions of 300 milligrams, which is half the suggested 600-milligram daily dose. A more accurate yearly cost would be $308,000. And the annual expense for a patient will probably rise since, as Dr. Belanoff noted in a recent conference call, Corcept expects the typical prescription to eventually be 730 milligrams daily, the dosage explored in the FDA study.
Taxpayers are playing a growing role in Corcept’s expansion plans. According to Medicare Part D coverage data, in 2016 (the most recent year for which statistics are available), the government forked out $23.1 million for 1,086 prescriptions in the United States, a steep increase from 2015’s $11.4 million expenditure. All told, Medicare Part D payments accounted for just slightly more than 28 percent of Corcept’s revenue in 2016, a jump from 14 percent in 2015.
Medicare Part D and the Department of Veteran Affairs records are the only two sources for the general public to search for details about who prescribes Korlym. People who rely on private insurers place their orders through a single specialty pharmacy, whose sales are not reported to prescription-monitoring services. According to Medicare Part D payment records, 44 doctors each wrote at least 11 Korlym prescriptions in 2016. (The Centers for Medicare & Medicaid Services doesn’t release the names of doctors writing 10 or fewer prescriptions.)
Eleven of the 15 doctors who are the most frequent prescribers of Korlym to Medicare Part D enrollees received at least $7,500 in speakers bureau payments from Corcept in 2016 and 2017 combined. (The centers’ Open Payments Data portal lists payments only to medical doctors and not physician assistants; its data for 2018 will be released in May, along with 2017 Medicare Part D data for Korlym.)
A savvy observer might suspect that Corcept is using its speakers bureau program to compensate doctors for prescribing Korlym.
To be sure, the concept of a speakers bureau is a fully legal, well-used strategy employed by many pharmaceutical companies. Done by the book, these programs serve both marketing and educational purposes: Doctors are compensated for their time in preparing presentations and discussing their experiences of administering a medication to their patients, and other physicians can hear a discussion about the drug at a level of sophistication that a sales representative would be hard pressed to match.
But in practice, as the Southern Investigative Reporting Foundation found after its investigation of Insys Therapeutics, speakers bureau programs (if not carefully monitored) can devolve into frequently questionable, if not illegal, quid pro quo inducements.
Note: PA refers to physician assistant. Source: Centers for Medicare & Medicaid Services
Another thing that stands out in the list of high-volume Korlym prescribers is their peculiar geographic clustering. Cushing’s syndrome is a rare disease. The FDA has estimated that the number of people in the United States who could be prescribed this drug is 5,000. So some medical experts might be surprised to see Korlym prescribers found mainly in small towns and modest-sized cities, many at a substantial distance from established medical research centers. (For example, Dr. John C. Parker, a Wilmington, North Carolina–based endocrinologist, wrote at least 41 Korlym prescriptions in 2016. But one would have expected instead that some larger-volume prescribers would be located, say, in the state’s heavier populated Durham and Chapel Hill area, where two pituitary disorder clinics are affiliated with prominent university hospitals. Wilmington, though, is about 2.5 hours by car from these clinics.)
Could these doctors based in smaller communities with a limited pool of patients to draw from be prescribing Corcept to patients merely with diabetes — instead of endogenous Cushing’s syndrome?
When Corcept’s CFO Robb was asked during the late December interview if his company was using its speakers bureau program to encourage doctors to prescribe the drug for off-label uses, he said the company was doing no such thing. He argued that the FDA’s estimate of 5,000 U.S. patients who could potentially take the drug was somewhat arbitrary and nearly seven years old. He said that a better figure, based on research by Corcept and Novartis, is closer to 20,000. (Novartis is in the late stages of testing its own Cushing’s syndrome drug.)
In addition, Robb said that as awareness of Korlym grows, doctors will realize that more of their patients have Cushing’s syndrome, and the clustering of Korlym prescribers in smaller communities happened only because one group of physicians recognized earlier than their colleagues how the disease could be treated.
Pressed on the unusual odds of so many prescriptions for a treatment of such a rare disease from doctors in Zanesville, Ohio and Murfreesboro, Tennessee, Robb declared that “over 90 percent” of all Korlym prescriptions were “on label.” He added that “since it’s an expensive drug,” nearly all commercial insurers have an extensive preapproval process before paying for the drug.
Speaking more generally about Corcept’s marketing efforts, Robb said a company has a lot of work to do when selling a medicine for a rare disease like Cushing’s syndrome. “It is just not the case that you can walk into a doctor’s office, drop off some brochures and come back later and suddenly they’ve got a Cushing’s syndrome patient. It takes five to seven visits” for physicians to become aware of the disease, he said.
“I know the meal [served during the presentation] is modest,” Robb added. “It’s held at your local Holiday Inn or whatever and it’s entirely compliant with the PhRMA code.” The code he referred to is a set of voluntary ethical guidelines for drug companies adopted in 2002 by the Pharmaceutical Research and Manufacturers of America, frowning on sales representatives using gifts to doctors or providing them meals or entertainment as a means of drumming up business.
“We’re not flying people to Hawaii to hear about our drug,” Robb said.
Robb’s full-throated defense of Corcept’s business practices would make more sense if not for the company’s relationship with Dr. Hanford Yau. An endocrinologist, Dr. Yau sees patients at an Orlando Veterans Administration Medical Center’s clinic.
According to records obtained by the Southern Investigative Reporting Foundation, Yau and his colleagues at the VA clinic prescribed Korlym for 84 people from early 2016 to Sept. 1, 2018. Yau wrote 27 of the prescriptions. A back of the envelope calculation, using 2017’s sales and prescription volume, illustrates how important the clinic is to Corcept: VA records from that year reveal that 50 people began taking Korlym through prescriptions written by the clinic’s doctors. With their medication costing the then-prevailing price of $290,304 a year (or $24,192 a month), these 50 patients generated more than $14.51 million in sales, or 9.1 percent, of the company’s $159.2 million in 2017 revenue. (Of course, some of those taking the drug in 2017 might have started only in the middle of the year. And the figure excludes patients who had already begun taking Korlym in previous years and stayed on the drug.)
Moreover, just as his clinic had become so central to Corcept’s economic well-being, Dr. Yau became the company’s leading recipient of speakers bureau payments. In 2017 he received $95,139 from the company — over 12 percent of Corcept’s total payments to medical professionals — a more than sevenfold increase from 2016’s $13,524, according to the Centers for Medicare & Medicaid Services’ Open Payment Data portal. (But in 2014 and 2015 combined, Yau was paid just $4,610.) The second leading recipient of the company’s speakers bureau cash in 2017 was Dr. Joseph Mathews of Summerville, South Carolina, who was paid $73,777.
None of these payments were for research purposes, according to the Open Payments Data portal. Nor does Dr. Yau’s name surface on ClinicalTrials.gov, the U.S. National Library of Medicine’s database of public and private clinical studies.
Asked several times about this doctor’s relationship to his company, CFO Robb would speak only in broad terms about the speakers bureau program’s goals without discussing Dr. Yau. He did not answer a follow-up question sent via email. And Dr. Yau did not reply to a phone message or email.
Through a Freedom of Information Act request, the Southern Investigative Reporting Foundation obtained emails between Dr. Yau and Corcept that show he was working with an Italian endocrinologist and another VA colleague to create a white paper for marketing Korlym to “community physicians.”
The expectation for a peer-reviewed medical journal article is that an investigator’s research is conducted independently from consultations with a drug’s manufacturer. But the emails obtained through the FOIA request, as shown in the image below, show that Corcept was entirely in control of this project conceptually and editorially. (The image also reveals where the VA redacted the name of the person directing the project for Corcept and other related identifiers.)
In addition, the fact that the Orlando VA Medical Center generates so many Korlym prescriptions is rather curious. The patient base of the VA’s medical system nationwide has in recent years been more than 91 percent male, according to the department’s analysis of those using its services from 2006 to 2015. But Cushing’s syndrome typically occurs in women rather than men, by an almost 5-to-1 ratio, according to the National Organization of Rare Disorders.
Susan Carter, a VA spokeswoman, did not reply to several calls and an email seeking clarification about Dr. Yau’s prescribing of Korlym and compensation for serving as part of Corlym’s speakers bureau.
Update: This story has been amended to include two paragraphs discussing the natural limitations of the FDA’s Adverse Events Reporting System and the Southern Investigation Reporting Foundation’s approach to reporting with this data.
Frequently sporting a $2 billion plus market capitalization, Acadia Pharmaceuticals brings to mind the work of Belgian surrealist Rene Magritte. His 1929 painting “The Treachery of Images” depicts a pipe with the inscription “This is not a pipe,” suggesting that an image and its meaning don’t necessarily correspond with each other.
In that vein, San Diego–based Acadia portrays itself as a pharmaceutical company but a Southern Investigative Reporting Foundation investigation has revealed that this is merely a clever facade. What lies below is a ruthless marketing entity whose pursuit of regulatory approval is best described as “loophole-centric.”
Nonetheless, in little more than two years, Acadia has gained a remarkable foothold in the pharmaceutical marketplace. The company generated $124.9 million in sales last year — a steep increase from its $17.3 million in 2016 — and its management has told brokerage research analysts to expect its revenue to more than double this year.
This is troubling since evidence is mounting that something is horribly wrong with Acadia’s sole drug, Nuplazid, an antipsychotic for Parkinson’s disease patients who experience episodic hallucinations and delusions. These are symptoms of a condition called Parkinson’s disease psychosis.
In April CNN uncovered a dramatic increase in the number of reports involving Nuplazid filed with the Food and Drug Administration’s adverse events reporting system. As noted in CNN’s reporting, an adverse event report does not mean that a drug is the cause of harm, but the document is used to help track possible issues.
In the wake of CNN’s story, FDA Commissioner Scott Gottlieb took the unusual step of telling lawmakers he would order his colleagues to “take another look” at the drug. In reply to a question about Gottlieb’s statement, Acadia sent the Southern Investigative Reporting Foundation a six-page press release from April 27 that asserted the FDA had not determined the drug posed a new risk and that doctors could continue to prescribe it.
Acadia has accomplished its growth in ways that have attracted intense regulatory scrutiny for other drug companies. The questionable practices include dispensing wads of cash to doctors to incentivize prescription writing and downplaying mounting reports of patient deaths.
————————
Central to Acadia’s marketing is promotion of the faulty illusion that Nuplazid received FDA approval like any other drug — after successfully passing a series of clinical trials and evaluations for the efficacy and safety of its target population. But that’s not the case: Nuplazid essentially tiptoed into the market through the FDA’s equivalent of the cellar door, a legal but unusual method of entry. In other words, the mounting fatalities reported by CNN — and the spiraling costs for the drug that Medicare and private insurance payers are reimbursing — would never have occurred if Nuplazid’s manufacturer had followed the FDA’s standard drug-approval practices.
To understand what’s happened consider how Acadia and Nuplazid fit into the spectrum of the pharmaceutical industry’s efforts to combat neurodegenerative illnesses like Parkinson’s disease. According to the basics of brain chemistry, the substantia nigra pars compacta is a part of the brain stem whose key function is producing dopamine. That chemical transmits and processes signals between the brain cells that govern the human motor function, memory and the response to pleasure. Parkinson’s disease greatly diminishes the production of dopamine, and the neural pathways that carry dopamine deteriorate to a point where motion is mostly inhibited, leading to the muscular shaking and trembling that are the illness’ hallmark.
There is no cure for Parkinson’s disease, and despite prodigious amounts of medical research few therapeutic prospects are on the immediate horizon, even as a gallery of once devastating afflictions — from polio to HIV — have become preventable and treatable. This is not for want of trying: A long list of pharmaceutical companies have spent billions of dollars on research and development of various remedies for Parkinson’s disease only to be forced to abandon their efforts as clinical testing has revealed a lack of efficacy or safety (or frequently both.) A 2014 article in Alzheimer Research & Therapy pegged the failure rate at 99.6 percent (or 243 of 244) for all the trials from 2002 to 2012 for drugs to treat neurodegenerative diseases.
(Yet a 2017 medical journal article, assessing recent developments in Parkinson’s research, took the view that some cautious optimism is warranted, however.)
Since the mid-1960s treating Parkinson’s disease has typically involved prescribing levodopa, an amino acid that when taken with carbidopa can stimulate the brain’s dopamine production and restore much of a patient’s normal muscular function. But these improvements are often temporary since the disease’s progression degrades the cells storing the newly made dopamine. And taking levodopa carries complications, since an elevated level of it has been linked to episodic hallucinations, anxiety and muscle tremors — the very symptoms patients need addressed.
Standard antipsychotic drugs offer little respite since they block the very dopamine receptors that are already in bad shape. And what’s more, the FDA has issued a so-called black box warning on this class of drugs due to the elevated risk of a stroke for elderly people with dementia.
Enter Acadia’s Nuplazid. Developed in the late 1990s, the drug was designed to stimulate a subset of the brain’s serotonin receptors, or the proteins that govern memory, cognition and learning. Relying on initial laboratory results, Acadia’s management argued that the drug should be able to lessen or eliminate the episodic hallucinations.
There was just one hitch: Nuplazid, when tested on people, has been a bust from the very start. The drugmaker has had a brutal time demonstrating that the medication works better than a sugar pill. For example, Nuplazid’s first clinical trial closed in March 2007, without any posting of results. The drug’s third trial ended in March 2014 but did not indicate any meaningful statistical difference between the medication and a placebo.
Statistically speaking, a drug trial whose range of results include zero is judged to be a failure in that the drug’s therapeutic benefits are deemed to be too small to be of medical consequence.
Faced with a third failure, Acadia’s management might have decided it had reached the end of the road in trying to successfully develop the drug. But due to a provision of the Food and Drug Administration Safety and Innovation Act, however, in August 2014 Acadia was able to get Nuplazid classified as a breakthrough therapy, a status conferred on therapies with “substantial treatment effects” in their initial clinical tests.
It was a curious decision, given Nuplazid’s track record and the FDA’s plainly stated requirement for a breakthrough therapy to have “substantial treatment effects observed in early clinical development.”
For the FDA’s part, Dr. Mitchell Mathis, the agency’s division director of psychiatry products, told the panel reviewing Nuplazid in March 2016 that awarding the breakthrough designation hinged on the fact that no other FDA-approved drugs existed for treating Parkinson’s disease psychosis, as well as the frequency that these patients were being placed in nursing homes, which he called “a harbinger of death.”
More baffling still was the FDA’s willingness to assess whether Nuplazid worked based on “a negotiated evidentiary standard” that eliminated long-standing evaluation criteria.
In a November analysis, Quarter Watch, a publication of the Institute for Safe Medication Practices, flagged several ways the approval process of Nuplazid was unusual. For example, the FDA permitted the drug’s efficacy to be measured against an index of nine psychotic symptoms — as opposed to the standard 20-point scale — and the patients in the study were exclusively advanced cases (the most likely to be responsive to any drug). The agency also allowed Acadia to stage only a single trial (rather than the usual two) and to run it just in North America, where its previous results had been marginally stronger.
The physician responsible for leading the FDA’s medical review of Nuplazid, Dr. Paul Andreason, recommended against the medication’s approval, asserting there was an “unacceptably increased, drug-related, safety risk of mortality and serious morbidity.” Andreason worked for 26 years for the U.S. Public Health Service until leaving it in 2016; he spent 13 years with the FDA. His no vote was unusual in that it publicly revealed fault lines inside the division over what constitutes an appropriate level of patient risk.
Presumably, Nuplazid would not have been given a breakthrough therapy designation if the FDA’s psychiatry product unit’s leadership thought the drug was unlikely to win approval. As ProPublica recently described, over the last several years the FDA’s approach to the review process for Nuplazid and a series of other drugs has shifted to active cooperation with pharmaceutical companies in getting their drugs commercially launched — and away from serving as a strict arbiter of science and as a guardian of consumer safety.
“The FDA’s division of psychiatry usually reviews drugs with an eye towards a lifetime of use,” said Andreason, in an interview with the Southern Investigative Reporting Foundation. “We rarely saw high morbidity in something under our consideration; [Nuplazid] is the first drug where a psychiatrist has to understand life is at risk.”
Andreason’s presentation to the FDA committee, summarizing the research he conducted and outlined in the meeting’s transcript, described Nuplazid’s results as presenting a “safety signal.” Specifically, 49 of the 459 patients who took the drug on a long-term basis either died during the trial or within 30 days of its completion. This represents a fatality rate that’s higher than 10.6 percent. For the placebo group, according to the FDA’s briefing document, the figure was 1 out of 210 in a key trial. For the 901 patients who took at least one dose of Nuplazid, the associated fatality rate was slightly higher than 5.4 percent. Andreason also observed that the patients taking Nuplazid had about a two-and-a-half-fold increase in the observed risk ratio — defined as reported incidents of an infection, a patient’s deterioration in mental clarity or death — when compared with the rate for those taking the placebo.
After weighing this evidence, the panel determined there was a lack of a “pathologically unique” identifier connecting Nuplazid to the 49 deaths. And given the fact that on average people with Parkinson’s disease may live only two to four years after the onset of psychosis, the panel did not classify the number of deaths among trial participants as unusual.
Dr. Andreason did acknowledge data that pointed to some patient benefit from Nuplazid. (There were 14 reported cases of people who took Nuplazid and showed remission from Parkinson’s disease psychosis versus a single reported remission among the placebo group.) But he told the panel that the FDA’s “usual logic” would require rejecting the drug.
And Dr. Andreason had company within the FDA in expressing concern over Nuplazid’s safety. As part of the briefing document prepared for the review panel, division of psychiatric products chief Dr. Mathis wrote a memorandum noting that while the drug’s trial was considered “strongly statistically positive,” he and some of his colleagues were hesitant to accept that the reported results were indeed “clinically meaningful,” especially in light of the drug’s “toxicity” and substantial safety risk.
“‘Does this drug work and is it safe?’ are what every medical reviewer is supposed to evaluate,” said Dr. Andreason. “And my answers were ‘not really’ and ‘no.’”
He said that his recommendation to reject Nuplazid represented a statement.
“I wanted my vote to be a clear signal that our past experience had been that the FDA had not [approved drugs with this safety profile] and that by discounting this data they would be making a real policy change.”
But his views didn’t sway a majority of the panel’s members; Nuplazid gained approval for commercial use on a 12 to 2 vote.
So why did Dr. Andreason’s colleagues overlook his arguments?
“The philosophy of our health care system has changed: People and doctors are taking a different stance than 20 years ago,” Andreason said, describing the emergence of a worldview stressing the importance of family and caregiver perceptions of the quality of life for a Parkinson’s disease patient. This shift, he said, demands that doctors do everything possible to help family members with their efforts to make their loved ones comfortable.
“This is a total shift from the culture in the 1970s and 1980s where the pressure was on doctors to avoid risks to patient health,” he said. “And it’s unreasonable to think the FDA wouldn’t be aware of these pressures.”
According to the transcript of the panel’s hearing, one of the two votes against approval came from the consumer representative, Kim Witczak, who has publicly stated that her interest in the psychiatric drug-approval process emerged after her husband’s 2003 death. (In her role as head of a medication safety organization she founded in 2004, WoodyMatters.com, Witczak has shared her view that a key factor in her husband’s death was several then undisclosed side effects of the antidepressant he took. She also told the Southern Investigative Reporting Foundation that Acadia complained to the FDA about her presence on the panel.)
In an interview with the Southern Investigative Reporting Foundation, Witczak explained she voted against approval because “I didn’t think it was a reasonable risk for patients given Acadia’s [presentation of] data.” She said, “And when I asked their doctors basic questions about how the company planned on preventing off-label use, they were evasive.”
Witczak continued, “For every two people who had a 50 percent reduction of psychosis, a third person had a severe reaction.” She added, “I asked [the FDA’s deputy director of clinical science], Bob Temple, if the FDA considered this a robust trial — on any level — and he said no.”
Nuplazid’s performance is suspect in another, more recent study, undertaken as part of Acadia’s attempt to gain approval to treat Alzheimer’s disease psychosis. (Such approval would be a boon for the company as a treatment for Alzheimer’s disease psychosis would represent a much larger potential market than one for Parkinson’s disease.)
In a Lancet Neurology study published in February, Dr. Clive Ballard, a faculty member and dementia specialist at Great Britain’s University of Exeter Medical School, said over a six-week period Nuplazid demonstrated “efficacy in patients with Alzheimer’s disease psychosis.“ But he neglected to point out that nearly all substantive tests on antipsychotics last 12 weeks.
In a commentary on the Ballard-led study that was commissioned by Lancet Neurology and published alongside it, Dr. Lon Schneider, bluntly dismissed Nuplazid’s prospects for treating Alzheimer’s psychosis.
“The results of this trial cannot be considered to be positive or clinically meaningful,” Schneider wrote about the 2017 study conducted at 133 nursing homes in England.
The trial wasn’t long enough, argued Schneider, a professor at University of Southern California’s Keck School of Medicine. “If the primary outcome had been specified for 12 weeks, typical of previous trials with antipsychotics,” he said, “then [Nuplazid] would have been considered as not effective.” (Ballard did state on the front page of his study that at the 12-week mark there was little difference between the drug and placebo.)
Reached for comment, Schneider said, “I’ve seen or heard nothing since the article’s release that points to [my] view being problematic.”
Yet, there’s an odd feature to the study: According to the study’s chart tracking patient responses, at the six-week point the reported results from the placebo and Nuplazid deviate. But before and after the six-week mark, the results from Nuplazid and those of placebo essentially mimicked each other, suggesting that the drug had a minimal effect on most Alzheimer’s psychosis symptoms. No explanation for this hiccup is apparent other than it being so-called noise, an artifact, or an error introduced at some point in the testing process.
The study measured results using the neuropsychiatric inventory for nursing homes, or NPI-NH scale, assigning points based on how well Nuplazid addressed standard Alzheimer’s psychosis symptoms. So the lower the score, the more favorable the reaction. For instance, if a patient’s difficulty in sleeping increased (or was unchanged) after starting to take Nuplazid, this case was assigned one point. If the sleeping difficulties improved, the score was zero.
The Southern Investigative Reporting Foundation posed several questions to Acadia about the Lancet Neurology paper — in February. The evening before this article went to press, the company provided the following response: “While we consider the findings from the study Dr. Lon Schneider referenced in the Lancet Neurology to suggest potential efficacy and acceptable tolerability of [Nuplazid] for psychosis in Alzheimer’s disease, we are currently conducting a well-controlled, confirmatory Phase 3 study in patients with Dementia Related Psychosis.”
————————
The upshot of the FDA panel’s approval of Nuplazid for Parkinson’s disease psychosis is that the drug is selling like hotcakes despite, as noted above, the unfavorable media scrutiny and the remarks from FDA Commissioner Gottlieb.
Bet on that changing, though.
Much of Acadia’s business model appears to have been built using as a template the methods of Avanir Pharmaceuticals, an Aliso Viejo, California-based, neurology-focused company with a pair of drugs currently on the market. (Avanir is owned by Japan’s Otsuka Pharmaceuticals.) Since April 2016 Acadia has hired 26 former Avanir staffers, with 22 of them serving as sales representatives: Ten of the 22 sell the drug primarily to nursing homes and other long-term care facilities.
Hiring Binge
Sources: LinkedIn and the Southern Investigative Reporting Foundation
If the name Avanir rings a bell, it may be because CNN’s October investigation found the company’s marketing strategy was medically and ethically dubious. The company’s drug, Nuedexta, treats a condition called pseudobulbar affect, a rare side effect of multiple sclerosis and Lou Gehrig’s disease resulting in sudden, uncontrollable bouts of laughter or crying.
Instead of peddling Nuedexta to the rare neurologist whose patient was experiencing pseudobulbar affect, Avanir’s sales staff found many physicians willing to prescribe it off-label to elderly people with dementia or Alzheimer’s disease. The investigation uncovered a close connection between the upward trajectory of Nuedexta’s prescription volume and Avanir’s payments to physicians for consulting and speaking fees.
Avanir’s off-label sales strategy initially increased the company’s revenue and propelled its stock price growth, from the drug’s November 2010 launch through the end of 2016. But adverse publicity after CNN’s October story weighed heavily on Nuedexta sales last year, with its $219.4 million total being about $55 million below management’s projections.
Source: Company documents
Dig into Avanir’s quarterly filings, however, and Nuedexta’s waning prospects appear in sharper relief. In the second quarter of 2017, sales of the drug totaled nearly $64.5 million. But in the first quarter of this year, its sales declined to $49.8 million.
A Centers for Medicare and Medicaid Services warning last month to insurers “about increases in [Nuedexta] utilization that may not be readily discerned or may relate to potential fraud” is sure to accelerate this downward arc.
Yet Otsuka management’s Nuedexta sales estimate for this year (made in February in the supplement to its annual financial filings) is more than $300 million, which would represent an increase of about 25 percent over 2017’s results.
Sources: SEC filings and company documents
Unlike Avanir, Acadia does not have a deep-pocketed parent to absorb the potentially steep costs should regulators and plaintiff’s lawyers begin to demand answers.
One area where Acadia has hewed closely to Avanir’s script can be found in the Centers for Medicare and Medicaid Services Open Payments data.
In a word, Acadia didn’t just open up its corporate wallet for doctors: It pointed a hose and sprayed cash at them.
Source: The Centers for Medicare and Medicaid Services’ Open Payments database
Over the six months that Nuplazid was commercially available in 2016, Acadia spent $609,556 on consulting, speaking and travel and lodging payments to 1,578 doctors: Pomona, New York, psychiatrist Dr. Leslie Citrome’s $25,690 payout amounted to the largest sum, followed by the $19,142 paid to Dr. Khashayar Dashtipour, a Loma Linda, California-based neurologist.
But what a difference a year makes.
For 2017, Acadia paid more than $8.6 million to 7,051 physicians, with 62 doctors receiving more than $50,000 apiece, and 26 receiving at least $100,000 each.
The leading recipient of Acadia cash last year was Dr. Neal Hermanowicz, an Irvine, California-based movement disorders specialist who took in $180,123, a handsome improvement over 2016’s $10,421. The runner up was psychiatrist Dr. Jason Kellogg, of Santa Ana, California, who was paid $166,259. (In contrast, the $25,690 that Dr. Citrome received in 2016, which was the biggest payout for that year, would have ranked as only the 104th largest payment to doctors if it had been given out in 2017.)
Given the fact that Acadia hired a significant number of former Avanir sales staffers, a substantial number of doctors have ended up receiving consulting payments from both Avanir and Acadia in the same calendar year: A total of 31 did in 2017, as did 29 in 2016. Out of that group, a dozen doctors took in $5,000 apiece or more from the two companies in 2017. Just six did in 2016.
Acadia’s payments in 2017, according to the Centers for Medicare and Medicaid Services’ Open Payments database, were almost entirely for consulting, save $522,935 for food and beverage expenses. (Other payment categories the centers track include “honorariums,” such as fees for lecturing to other medical professionals, or “education,” when the company covers the expense of distributing a journal article or staging a presentation at a conference.) Despite Acadia’s discussions about supporting research on Nuplazid, the company’s appetite for external or independent research sharply declined last year. It spent just $197,587 on doctors’ research projects, in contrast with its $817,613 outlay in 2016. (Avanir went in the other direction, devoting $7.61 million to research last year and $4.36 million to payments to doctors.)
Since Acadia doesn’t release Nuplazid’s prescription count, Medicare Part D data is the only way to observe prescriber behavior. To that end, overlaying Medicare Part D prescription volume from 2016 (the latest period for which data is available) against the Centers for Medicare and Medicaid Services Open Payments data for 2016 and 2017 illuminates a few things.
There’s a good deal of overlap between those who received Acadia consulting fee payments in 2016 and 2017 and the individuals who prescribed Nuplazid with some frequency in 2016. For instance, in 2016, 14 of the 25 most frequent prescribers of Nuplazid to patients covered by Medicaid Part D received “consulting fees” in 2017 worth more than $1.21 million in total.
Almost 37 percent of Acadia’s $1.21 million in consulting fee payments, or $443,014, went to three neurologists who conducted Acadia-funded studies on Nuplazid and published journal articles about their findings: Dr. Neal Hermanowicz; Dr. Stuart Hal Isaacson of Boca Raton, Florida; and Dr. Rajesh Pahwa of Kansas City, Kansas.
Pittsburgh-based Dr. Susan Baser, a leading prescriber of Nuplazid to patients paying for it via Medicaid Part D, told the Southern Investigative Reporting Foundation, “It’s the only drug addressing [Parkinson’s disease psychosis] and we’ve had positive effects in some patients.” She added, “Personally I think it’s a good drug despite the noise about adverse events that’s out there.”
Baser, who did not receive any consulting fees from Acadia in 2016 and 2017, expressed surprise at the size of the payments that some of her peers received from the company. “I work 60 hours per week. I don’t know how they have the time. I’m just too busy for any of that.”
In addition, despite its skyrocketing sales, Nuplazid appears to have had some challenges in gaining traction among the neurologists and psychiatrists who treat Parkinson’s disease and other movement disorders. According to a review of data for all Nuplazid prescriptions paid for by Medicare Part D, 2,020 doctors or other medical personnel wrote at least one prescription for the drug in 2016. (The Centers for Medicare and Medicaid Services doesn’t list the names of individuals who write fewer than 11 prescriptions, due to patient-privacy concerns.) Only 170 doctors or other eligible prescribers wrote at least 11 prescriptions.
Of those 170 prescribers in 2016, 13 were either nurse practitioners or physician assistants whose payments from pharmaceuticals companies are not included in the Open Payments system. Among the remaining 157 individuals, 70 did not receive any money from Acadia in 2017. This suggests they may not have continued to write enough prescriptions for the drug in 2017 to draw attention from the company. (Some of the 157 individuals may have refused consulting fees or honorariums because of scheduling constraints. But current and former sales staffers for pharmaceutical companies told the Southern Investigative Reporting Foundation that these businesses aggressively try to maintain long-term connections with the most frequent prescribers.)
Acadia told the Southern Investigative Reporting Foundation that less than 5 percent of Nuplazid’s prescriptions come from its top 10 prescribers.
————————
The money behind Nuplazid is only its second most compelling characteristic. The first is the sheer number of medical issues that appear to be linked with the drug’s use.
According to the FDA’s adverse events reporting system (FAERS), from January through the end of March, 162 patients have died while taking Nuplazid. The figure is 612 since the drug’s June 2016 debut through this March. Those fatalities, however, are just part of a larger picture that suggests longer-term challenges for Acadia: Since June 2016 nearly half of the 6,800 FAERS reports refer to topics like “hallucination” or “confusional state” or “drug ineffective.”
In response to questions on the FAERS data, Acadia investor relations representative Elena Ridloff responded via email: “Based on the totality of available information, ACADIA is confident in Nuplazid’s efficacy and safety profile which remains unchanged and — as the FDA itself has stated — is appropriately described.”
These adverse event reports aren’t considered as conclusive as an official autopsy, and the fact that a patient died while taking a certain drug doesn’t mean the medication caused it. Also, this completely voluntary reporting system allows for a wide array of filers. Family members, caregivers and trained medical professionals can make submissions. So the level of accuracy and detail can vary widely. Finally, many medical professionals have suggested that because this documentation is voluntary, many incidents involving drugs are not reported to FAERS.
An analysis of the longer-form FAERS case reports — obtained via Freedom of Information Act requests — illuminates Acadia’s success at getting prescribers to order Nuplazid for patients within long-term care facilities. The majority of the adverse events for these patients involved off-label use of the drug for various dementia-related psychoses, despite the explicit black-box warning.
A notable feature of many of the individual case reports that documented a death is the brevity of the patient’s experience with Nuplazid. Given the spotty information found in many reports, though, it’s difficult to arrive at precise numbers overall. But for those case reports citing a death that also provided a time frame for the patient’s treatment with Nuplazid, exposure to the drug had been less than 90 days on average.
For example, a 75-year-old man, identified only as Case ID: 12689689, began taking Nuplazid on Aug. 3 2016. By Aug. 26 he was dead. His cause of death was listed as “unknown,” but the case report said he had been diagnosed with Parkinson’s disease dementia.
(Nuplazid, like many similar drugs, has been observed to have a mild but discernible effect on the electrical cycle of the heart’s ventricles — in a process that cardiologists call repolarization and depolarization. Think of it as being like the movement of a swing: Depolarization is when the swing goes down; repolarization is when it heads up. The measurement of the length of the time between the two is called the QT interval, or “the space between the start of the Q wave and the end of the T wave,” according to the Mayo Clinic. If the QT interval is prolonged, the possibility of an arrhythmia sharply increases.)
Some other concerns about Nuplazid can be understood through the history of Case ID: 13253142. This 91-year-old man was (despite the black box warning) prescribed the drug to treat his Parkinson’s disease dementia and psychosis. He began taking Nuplazid in November 2016 but soon stopped for a five-month period after reports of sleep disruption and a loss of mental clarity; the report isn’t clear about whether the prescriber stopped the treatment because of this. In April 2017 the elderly patient resumed taking the drug again; soon afterward medical personnel reported that he began entering into catatonic states. After a series of health problems, including rapid weight loss and the inability to swallow, he died in May 2017. (The attending physician and the patient’s son blamed factors other than Nuplazid for the man’s death, such as the poor quality of care in his assisted living facility.)
To gain a sense of how Nuplazid’s number of adverse event reports compares with other Parkinson’s disease-focused drugs, the Southern Investigative Reporting Foundation used the FAERS database to create two charts. If Nuplazid’s death rate was parallel to other Parkinson’s drugs, the explanation for it would be unlikely to be drug-related; alternately, if those taking Nuplazid died more frequently than the comparison group, re-visiting the drug’s safety profile would be logical.
The first compares the number of serious incidents and deaths reported for people taking Nuplazid with the tally of serious incidents and deaths for individuals taking nine other Parkinson’s disease medications; the time frame considered was from June 2016 through the end of this past March. The nine other medications have longer track records for the treatment of Parkinson’s disease.
Nuplazid Compared With Its Peers
Source: The FDA’s adverse events reporting system
Reports uploaded to the FAERS database that indicate a patient died while taking Nuplazid sharply outnumbered the reported deaths of those on the nine other drugs: A total of 610 individuals died while taking Nuplazid but just 87 died while taking any of the nine other medications. Nuplazid-tied deaths represented more than 38 percent of the total number of serious incidents; but for those taking any of the other nine medications, death amounted to less than 5 percent all serious incidents.
These results cannot be interpreted as definitive: Patients taking Nuplazid are usually quite frail since they have had Parkinson’s disease for several years and might be weaker on average than the people on the nine other drugs. Additionally, newer drugs tend to draw more FAERS submissions than more established ones.
But these results certainly show Nuplazid has a radically different safety profile than other Parkinson’s disease treatments.
A second chart explores whether Nuplazid’s seemingly high level of adverse event reports is similar to reactions to another central nervous system-targeted drug, Namzaric, which was approved in 2014 for treating Alzheimer’s dementia.
A few variables are skewed in Namzaric’s favor. There is a high probability that the Alzheimer’s dementia patients who take Namzaric are frailer than the people being given Nuplazid. Also, Namzaric’s parent company, Allergan, has spent more than four years and tens of millions of dollars on advertisingonline and on television to raise the drug’s profile.
It stands to reason that a new, high-visibility drug like Namzaric would, if warranted, receive a great deal of adverse event submissions.
As the chart below shows though, it hasn’t: The number of reports of fatalities and adverse events associated with Nuplazid is much greater than that for Namzaric.
Nuplazid vs. Namzaric
Sources: The FDA’s adverse events reporting system and the Southern Investigative Reporting Foundation
Calculating the number of deaths as a percentage of the number of adverse events associated with the rate for Namzaric is tricky because few people who took either drug did so for the same amount of time.
Fortunately medical statisticians can rely on a measurement tool called “patient years.” It is an average of how many patients have taken a specific drug over the course of a given year. For example, assume a certain drug costs each patient $10,000 a year to take and that the medication had $100,000,000 in sales. Using the patient years calculation, researchers could say that roughly 10,000 patients took the drug for one year.
For this chart each drug’s annual sales figure was divided by its retail price at the end of 2016 and 2017: Namzaric cost $4,249 at the end of 2016 — and $5,069 in 2017. For Nuplazid, it was $25,000 and $33,336, respectively. Namzaric’s patient years figures in 2016 and 2017 were 13,536 and 25,805; Nuplazid’s were 692 and 3,747.
“Deaths per patient year” is a rough statistical way of measuring patient deaths while assuming the typical patient used the drug for a full year. Epidemiologists call this “the excess death rate,” or the number of deaths above what is reasonably anticipated in a population group.
The number of patient deaths for Namzaric was a scant .0001; Nuplazid’s tally, however, was .0881 in 2016 and .1033 in 2017.
So in 2016, if 1,000 patients took Nuplazid for one year, about 88, or 8.8 percent, could be expected to die over and above the already steep mortality rate of approximately 25 percent; in 2017 the figure would rise to 103. But it would take 10,000 patients on a Namzaric protocol for a full year for a single death to result.
This is the full text of Acadia’s response to the Southern Investigative Reporting Foundation’s questions.
Editor’s note: To obtain the fairest profile of the drug histories, the Southern Investigative reporting Foundation used adverse event reports of “serious cases,” or incidents that required medical attention, and then deaths were subtracted from this total. For the death figures, only deaths reported as a prospective reaction to a drug were counted, as opposed to the higher “death cases” figure that the FDA records.
Correction: An earlier version of this story inaccurately described Nuedexta’s safety profile. It has never carried a black box warning. Also Avanir Pharmaceuticals has two drugs that are commercially available.
Valeant Pharmaceuticals International, the corporate poster child for price-gouging, tax-inversion and hedge-fund manager wealth destruction quietly severed all ties with J. Michael Pearson, its former chief executive officer and longtime guiding light, in January, according to its annual proxy statement filed this morning.
While Pearson stepped down from Valeant in May 2016, and struck a wide-ranging separation agreement that paid him $83,333 per month for consulting — especially the much-touted and at least temporarily disastrous Walgreens contract — his primary job was to cooperate with the seemingly eternally expanding roster of civil and criminal investigations.
The deal with Pearson was supposed to last through this December and the use of the word “initial” in the contract’s wording was a suggestion it might be renewed. Valeant, in the proxy, says it last paid him in October, and in December its board of directors determined no more payments would be made: “In December 2016, the Board determined that we are not in a position to make any further payments to Mr. Pearson, including in connection with his then-outstanding equity awards with respect to 3,053,014 shares.”
Pearson’s agreement was terminated in January for unspecified reasons.
Assuming that Valeant’s language is not implying that the company simply doesn’t have the cash available to pay Pearson, then a legitimate question becomes whether he did anything to violate the terms of his agreement through noncooperation. Given that it paid him $1 million annually with full benefits, allowing him to have an office, an assistant and legal fees paid for, this does not seem to be in his best interests.
Also of note is the timing of the cessation of payments to Pearson in October given that charges against Philidor Rx Services were filed on Nov. 17. While it is highly unlikely that Valeant’s board would have a sense of when — or even if — additional charges might be brought, their own counsel was assuredly aware that federal prosecutors have a long-standing practice of refusing to negotiate settlements with companies where they are actively pursuing indictments against current leadership.
(Southern Investigative Reporting Foundation readers will recall its investigative work from October 2015 that began an ongoing reexamination of the company’s ethics and business practices that has forced its share price to $10.86 in recent trading, down from over $257 in July 2015.)
A call to Scott Hirsch, Valeant’s communications chief, seeking comment was not returned.
With Valeant Pharmaceuticals’ evolution from battleground stock to full-bore Wall Street circus, it is easy to forget that underneath the competing valuation narratives and regulatory drama is a real operating company.
The odd thing is that down at the operating level — where drugs are made, shipped to market and sold — things don’t get very much clearer.
One of Valeant’s more enduring riddles is the continued vitality of Wellbutrin XL, a drug that has been off patent since 2006. A January Bloomberg News article ably laid out Valeant’s strategy of constantly raising prices on the drug — 11 times since 2014 — that underscores how revenue jumped.
But looking at Wellbutrin XL’s prescription count data from the second and third quarters last year — specifically the reported revenues — some unanswered questions remain.
For instance, the third-quarter Wellbutrin XL prescription data captured by Symphony (and available via a Bloomberg terminal) indicated that the count declined by 2,743 prescriptions, to 67,312 from 70,055.
The decline in Wellbutrin XL’s prescription count makes plenty of sense since there are numerous factors working against the brand — the aforementioned price increases and additional generic competitors hitting the market after the Food and Drug Administration put to rest bioequivalency concerns.
What doesn’t make sense is how revenues increased 37.3 percent sequentially, jumping to $92 million from $67 million. It seems we can rule out Direct Success, the Farmingdale, New Jersey-based specialty pharmacy that fills Wellbutrin XL prescriptions for low (or no) patient co-pays and then works to secure reimbursement, as the channel for the difference.
While Direct Success is the obvious candidate to explain any discrepancies since data reporting services don’t capture specialty pharmacy prescription activity, Valeant itself ruled this possibility out when spokeswoman Laurie Little told Bloomberg News, “[Direct Success] accounted for less than 5 percent of Wellbutrin XL sales.” She also remarked that there were other channels where the drug is sold, including “Medicare, Medicaid and the Department of Defense.”
It is very unlikely that these channels factor into the Wellbutrin XL issue. Centers for Medicare & Medicaid Service contract awards are heavily contingent on price and the Department of Defense even more so; many Medicare Part D plans don’t even cover the brand. Here is a DoD contract out for bid, for example, and here is the (generic manufacturing) winner.
(As the Southern Investigative Reporting Foundation was finalizing reporting on this article, Wells Fargo research analyst David Maris released a report that mentioned Wellbutrin XL’s unusual performance in the third quarter of 2015, among numerous other issues. While ordinarily it would be unusual to be beaten to the punch by a sell-side analyst, Maris is an exception, having — ironically — caught Valeant’s corporate forbear Biovail Pharmaceuticals in a revenue inflation scheme. In full disclosure, I also reported frequently on Biovail, a legendarilycloggedcorporate toilet.)
One area that merits consideration is some sort of channel stuffing, wherein distributors are sold more drugs than they can presumably sell themselves.
Consider pharmaceutical distributors, who have very narrow operating margins (given the nearly riskless nature of their business) and whose business model benefits mightily from distributing drugs where price increases are regularly announced. This allows them to purchase drugs in advance of the scheduled increase and profitably resell them at a higher price.
For a manufacturer, aggressively moving extra inventory into distribution channels bears little risk: The profit on incremental volume moved is huge and it is effectively zero-interest financing since the company gets cash up front and simply return it to the distributor if product is unsold. The risk is that a manufacturer’s distribution networks have too much of a product and sales decline until inventories clear out. To be sure, there is a long history of pharmaceutical companies improperly handling the accounting related to drugdistribution.
Inventory reduction has certainly been on Valeant management’s mind.
At a December analyst meeting in Newark, then-chief executive officer Michael Pearson spoke about “bringing down the inventories in the wholesale channel,” “the continued impact of the reduction in channel inventories” and referenced getting “normalized in 2016.”
Valeant’s days sales outstanding do appear high as the chart below indicates, even adjusting for the inventory that came on balance sheet in April when the Salix purchase closed. (In December, the Southern Investigative Reporting Foundation released an investigation into Valeant’s unusual Eastern European distribution practices.)
Sources: Bloomberg and SEC filings
On Friday afternoon the Southern Investigative Reporting Foundation submitted questions via email to Valeant outside spokeswoman Renee Soto of Sard Verbinnen & Co. She did not reply by press time.
Shortly before 11 p.m. on Feb. 4, Valeant Pharmaceuticals CEO Howard Schiller took off from Dulles International Airport for home. It had been a long, tiring day of preparation, congressional testimony with plenty of blunt questioning and afterward came the inevitable debriefing with his legal and public relations advisory team.
It was not a lost day, though: Speculators in Valeant’s shares perceived Schiller as having done well and the stock price closed up $3.87, an unexpected development when a CEO is called to account for his company’s business model. He certainly helped his cause when he flatly admitted the company made mistakes and understood the pain its drug pricing policies had caused.
To be sure, it did not go flawlessly — there were several broadsides landed from the likes of U.S. Rep. Elijah Cummings, the head of the House Committee on Government Oversight and Reform panel that subpoenaed him. And a day earlier the Democratic committee staff had posted a letter — culled from discovery in the Committee’s ongoing investigation — with several deeply unflattering references to Valeant’s business practices.
Still, whatever else that day brought Schiller, it can be safely assumed that had the representatives known he flew home on Valeant’s G650, the world’s most expensive private jet, not even sitting next to a smirking Martin Shkreli — whose colleague was castigated for acknowledging Turing Pharmaceuticals threw a $23,000 party for its sales force on a yacht — could have shielded him from some populist outrage. (Congress has a track record of criticizing executive’s private jet flight at companies under investigation.)
This is Valeant’s G650:
So Schiller’s flight home was good. He did not have to sit on plastic seats waiting to be boarded by zones; he just walked right onto the plane. Nor did he have to shimmy into a closet-sized restroom that smelled like a mashup of Lysol and Mennen Speed Stick. There was plenty of leg room and he was always free to move about the cabin. In case he wanted a snack, the refrigerator has its own IP address that communicated its inventory to the D.C. based ground crew who restocked it prior to takeoff.
Exactly 57 minutes after takeoff Schiller landed at the Morristown, New Jersey, airport, a 20-minute car service ride to his home in Short Hills. Flying home at over 500 miles per hour, Valeant’s newly appointed CEO went from Dulles’ suburban D.C. tarmac to his northern New Jersey house in less time than he would have been inside an airport prior to boarding a commercial flight.
Flight records reviewed by the Southern Investigative Reporting Foundation suggest Schiller has quickly grown fond of the G6, having flown three times in the past month with his family and friends to a small regional airport in Montrose, Colorado, near his Telluride ski house.
Those drug pricing policies that necessitated Schiller’s D.C. interlude have made Valeant a great deal of money, or at least enough to maintain a fleet of three Gulfstream jets: a G4, G5 and G6. The G5 and G6 are owned through a company subsidiary, Audrey Enterprise LLC. It keeps them in Morristown, 23 miles away from its U.S. headquarters in Bridgewater.
Valeant is hardly alone in having a fleet of its own planes but it certainly chose from the high end of the menu. The G6 cost just under $65 million when it was delivered in 2013 and the G5 was about $59 million in 2012. It costs between $2 million and $3 million annually to staff, insure, house and maintain the three jets before variable costs like fuel — a 1,000-nautical mile trip in the G6 uses about 860 gallons — and cabin crew. When under way, the cost per hour is about $4,500 for the G5 and G6 and around $3,400 for the G4, although the recent drop in fuel prices probably puts these figures on the high side.
Under the best of circumstances a company extending its leadership the personal use of a major corporate asset like an aircraft can be fraught with potential headaches. At the top of that list is what happens when that company comes in for some bad publicity; then there is what happened to Valeant, which has become a corporate pariah.
Most chief executives would be hard-pressed to afford regular personal travel aboard a Gulfstream or its equivalent but Schiller’s personal financial situation is not like most chief executives. A Goldman Sachs partner at the time of its 1999 initial public offering — where his 0.375 percent stake became $61.87 million in cash — chartering his own plane isn’t likely beyond his means. His salary is $4.8 million and he currently holds a little over $36 million in Valeant shares.
Valeant’s 2014 proxy statement explicitly permitted Schiller’s predecessor Michael Pearson — who is still on medical leave and recuperating in his New Vernon, New Jersey, home — to use company aircraft as he saw fit. In 2014 it valued this use at $195,614 (although it stopped paying his taxes for these flights.) Schiller’s employment agreement does not mention aircraft use but in the proxy he and Pearson were the only executives with personal use allowances.
On Friday a Valeant spokeswoman, Renee Soto of Sard Verbinnen & Co., was emailed a pair of questions about “the optics” of flying back from the congressional hearing on a G6 as well as Schiller’s personal use of company aircraft. She did not reply.
Valeant Pharmaceuticals is the type of company that tends to make even the simplest things complex.
The contract of Howard Schiller, its new chief executive officer, is proof of this tendency.
On Jan. 6 Valeant’s board of directors gave Schiller the role of interim CEO; the company previously had an hoc, three-man “office of the chief executive”created on Dec. 28 in the wake of the disclosure that founder and then CEO J. Michael Pearson had taken a medical leave of absence of indefinite duration.
Notwithstanding the fact that Valeant has become the most closely followed company in the capital markets — attributable in part to the Southern Investigative Reporting Foundation’s revelations of its hidden ownership of Philidor — it was reasonable to have expected a filing several days after Schiller’s appointment that disclosed relevant compensation package details.
But that announcement came only on Feb. 1, three weeks after Schiller assumed control.
Schiller’s July 17 separation agreement sheds some light on why he ran a besieged company for over three weeks without an employment agreement in force. Recall that the then CFO resigned in April (after the high-profile Allergen acquisition bid collapsed) to pursue other interests.
The July agreement paid Schiller $2,500 per month for consulting and allowed 100,000 “performance restricted stock units” to vest on Jan. 31, 2016, giving him over $9 million worth of reasons to work (temporarily) for less than the salary of an assistant manager at a fast food restaurant. Each unit converts into one freely tradable share.
Why Valeant would not state that Schiller’s employment agreement would be disclosed after his 100,000 units vested is unclear. An email seeking comment from the company’s public relations adviser, Sard Verbinnen’s Renee Soto, was not responded to.
From a narrow point of view, Schiller’s new contract appears fairly standard; it paid him $400,000 per month for a two-month term ending on March 6. What happens then, however, is unclear. It certainly opens up a Russian nesting doll of questions: Is Michael Pearson seeking to return? If so, will there be disclosure about the root causes of his multi-month absence? If he can’t or won’t return, what criteria is the board of directors using to evaluate Schiller over a 60-day period?
Despite Schiller’s having $9 million in salable stock and a handsome salary on top of that, the money is unlikely to be much comfort for Schiller, given the looming date of his Feb. 4 for his appearance before the House Government Oversight and Reform Committee to answer questions about Valeant’s drug pricing strategy A Feb. 2 memorandum from the committee’s Democrats suggests that Schiller’s welcome will not be a warm one. Containing some unflattering excerpts culled from the more than 75,000 documents Valeant produced in discovery, it shows, among other things, that the company pursued transactions simply for the ability to raise prices. The memorandum did not try to hide the Democrats’ contempt for Pearson, mentioning him eight times in the seven-page document.
Corrections: The initial version of this story misstated the value of Howard Schiller’s restricted stock unit grant and inaccurately connected him to Valeant’s brief-lived office of the chief executive. The story has been corrected and updated.
Executives at Insys Therapeutics have continued to pressure its employees to develop new ways to mislead insurance companies into granting coverage to patients prescribed its drug Subsys, even as the Food and Drug Administration’s Office of Criminal Investigations is issuing a stream of subpoenas to former employees.
As reported in a December Southern Investigative Reporting Foundation story, Insys’ prior authorization unit (also known internally as the insurance reimbursement center) employees were trained and rewarded for saying anything, including purportedly inventing patient diagnoses, to get Subsys approved. The revelations illuminated the answer to the conundrum raised in our previous stories: How does a company marketing a standard fentanyl spray formulation, under a strict FDA usage protocol, easily double the insurance approval rates of its more established competitors?
Internal Insys documents and an audio recording of a prior authorization unit meeting show that as recently as the late autumn executives were frantically brainstorming new ways to get around increasingly stringent pharmacy benefit manager rule enforcement.
“[Pharmacy benefit managers] had begun to deny Insys’ [prior authorization] requests in the early autumn to the point where it was rare to get more than two dozen approvals per week for the unit,” said ex-prior authorization staffer Jana Montgomery (a pseudonym) and something that began to accelerate after the CNBC reports came out.
“That’s a big change from each employee getting 25, at least, per week.”
Unlike their sales unit colleagues, Insys prior authorization staffers can’t call on long standing professional relationships with prescribers or use speakers program cash to win business. They are hourly workers — albeit among the higher paid prior authorization staff in the medical industry — dealing with other hourly workers and both have little latitude to depart from established scripts. If the pharmacy benefit manager denies the coverage, Insys has few levers to pull, apart from beginning an appeals process.
As critical reports began to pile up in the press, particularly a November CNBC investigative series — and with at least a half-dozen state and two concurrent federal investigations ongoing — insurers began to deny authorization for Subsys.
By the spring Montgomery said that it was clear to everyone in the unit that something had to change or the business would grind to a halt. One big problem was that insurers appear to have gotten wise to what was known internally as “the spiel,” a script of dubious answers to pharmacy benefit manager employee questions designed to clearly suggest the patient had been diagnosed with breakthrough cancer pain (while not coming right out and saying so).
Put bluntly, with state and federal subpoenas becoming a common occurrence, the prior authorization unit could no longer afford to push the legal limits of word games. On the other hand, simply reporting an off-label diagnosis was an unpalatable option given that under 3% of Insys’ patients had cancer.
So Jeff Kobos, the prior authorization unit’s new supervisor, wrote a new version of the spiel that was alternately called “Statement 13” or, in a homage to its confidential nature, “Agent 14.” It tried to thread a needle, designed to navigate both elevated pharmacy benefit manager scrutiny and the rising level of compliance oversight required, while still allowing the unit’s employees to try and guide pharmacy benefit managers to an approval.
The problem being, according to Montgomery, is that the prior authorization unit had gotten behind the curve.
“If you’re doing a prior authorization it should always be straight forward and exactly what the provider gives you,” she said. Pharmacy benefit managers “learned to approach [Insys] with questions that had non-negotiable answers like, ‘On what date did the patient receive their original cancer diagnosis?’
“We didn’t figure that out right away and kept on submitting requests for authorization which were all quickly rejected.”
So like many corporate outfits the world over, the prior authorization unit held a meeting to discuss how to get better results (where “better results” was defined as getting people to think patients with back or leg pain had cancer.)
The Southern Investigative Reporting Foundation obtained a recording of this meeting, held in November.
The initial speaker (and the clearest voice) is prior authorization executive Jeff Kobos who makes a pair of important admissions: At the 2:20 mark he acknowledged the unit’s pattern of dishonesty by saying “when we were using [insurance codes for cancer-related pain diagnoses] for non-cancer [pain].” At 4:30, he made jokes referring to “sandwiches” and “the sky is blue” as the kind of conversational gambits they should try to deflect pharmacy benefit manager worker questions with.
At 5:00, David Richardson a trainer with the prior authorization unit, suggests dropping the “Agent 14” spiel since it wasn’t working. A minute later, he and his wife, Tamara Kalmykova, an analyst with the prior authorization unit, begin to discuss an idea he had in response to so-called smart-scripting, whereby employees of a pharmacy benefit manager use software analysis to determine if a patient — per the FDA’s protocol — had tried another fentanyl drug.
(Montgomery said smart-scripting was another development that Insys’ prior authorization staff couldn’t readily steer around.)
Richardson suggested patients use a coupon for a free-trial prescription of Cephalon’s Actiq. The patient wouldn’t pick the drug up but it would register in databases and allow prior authorization staffers to plausibly claim that the patient was in full compliance with regulations.
But smart-scripting wasn’t the only new obstacle that unit staffers were encountering. Humana, Silverscripts Medicare and other pharmacy benefit managers started requiring not only Actiq or Depomed’s Lazanda, a nasal spray, but the previous use of other major painkillers like morphine, oxycodone and hydromorphone. Still others were calling prescriber offices and confirming every aspect of the diagnosis, including prior history with fentanyl and other opioids.
Adding in a variable like the delivery system (lozenges, nasal spray or inhaler) did offer Insys an opportunity to claim that its patients could only tolerate oral inhalers. Montgomery said pharmacy benefit manager questions about prior use of Lazanda, for instance, were handled by noting the “provider states patient cannot tolerate inter-nasal spray.”
Unfortunately for Insys’ shareholders, the hard line taken with its prior authorization unit is having a very real effect on prescription count, according to IMS Health data.
Source: IMS Health
The number of Subsys prescriptions filled in the third quarter dropped about 4 percent from second quarter levels and the erosion accelerated in the fourth quarter, falling an additional 11%.
Thus far in January, the new year has not brought much in the way of promise, with the 815 prescriptions reported for the week ended Jan. 15 down 6 percent from the comparable week a year ago. Subsys’ share of the transmucosal immediate release Fentanyl market, which hovered near 50 percent for most of the summer, has now fallen below 45 percent.
————————
Jana Montgomery was given a pseudonym because of her cooperation with an ongoing federal investigation. Her account of prior authorization unit practices was read to two of her former co-workers who agreed with her characterization of “the spiel” and declining pharmacy benefit manager authorizations.
As is the case with prior Southern Investigative Reporting Foundation investigations, everyone named in the story was called repeatedly on mobile or home phones and left detailed messages about what we sought comment for. When possible an email was sent as well. As of publication, no one replied.
A detailed message was left on Insys general counsel Franc Del Fosse’s mobile phone seeking comment on these subjects. As of press time the call had not been returned.
The Insys that investors loved and that made its founder and chairman John Kapoor a billionaire is going away and, despite heroic efforts by company officials to rebrand it as a research and development-driven shop, its future will probably be less profitable, with little of the mercurial growth and compounding profits that defined its first four years.
The Southern Investigative Reporting Foundation interviewed two dozen then-current and former Insys Therapeutics sales staff, as well as six doctors and their staff, and their accounts paint a uniformly grim picture of the company’s prospects.
Its forecast is murky because the number of prescriptions for Subsys, Insys’ sole commercially viable product, is dropping and likely to continue to do so.
The forces arrayed against Insys, from a federal grand jury investigation in Boston to, as described in a Dec. 3 Southern Investigative Reporting Foundation story, mounting insurer scrutiny of Subsys prescriptions, represent brutal, if not possibly insurmountable, obstacles. A quick glance at Insys’ financial filings from 2012, when it was committed to marketing primarily to oncologists, is proof that playing by the rules is not very lucrative.
IMS Health data through late November, though, shows a 10.4 percent decline quarter to quarter in Subsys prescriptions. Even allowing for the traditionally soft Thanksgiving week, this is a grim trend for a company that regularly receives about 99 percent of its sales from Subsys.
Source: IMS Health data through Nov. 27, 2015
Dan Brennan, Insys’ new chief operating officer, seemed to reference the drop-off when he tried to rally the troops at a Dec. 3 analyst presentation by alluding to some unspecified “commercial opportunities . . . that can stabilize and grow scripts.”
Insys’ decidedly mixed third-quarter earnings report offered a clear sign of the company’s headaches. The seemingly impressive third-quarter revenue figures were boosted by $6.6 million in distributor shipments, which risk “stuffing the channel,” decreasing future sales and profits. More positively for the company’s prospects, lower unit demand of about 5 percent was offset by an $8.4 million gain from diminished rebate amounts and higher drug prices.
Absent this $8.4 million benefit, Insys would not have been able to report $91.3 million in revenue, allowing it to claim that it had beat the brokerage community’s $83 million consensus estimate.
Flagging sales, however, are nothing compared to what the looming Department of Justice settlement negotiations might bring.
Ready comparisons for Insys’ situation are hard to come by. The only analogy might be Purdue Pharma’s 2007 $600 million settlement with the Department of Justice for intentionally misbranding OxyContin. (Three Purdue Pharma executives also pleaded guilty and separately paid a combined $34.5 million in fines.)
Brokerage firm analysts expect Insys to pay a fine and perhaps agree to amended business practices, a standard ritual over the past decade for U.S. businesses accused of wrongdoing. Despite some shockingly large fines and settlement, especially for pharmaceutical firms, the process of writing a huge check and issuing a guarded, conditional apology (without admitting or denying anything specific) is made more palatable for companies as investors often bid up their share prices on the view that “the bad news is now behind them.”
Research by the Southern Investigative Reporting Foundation suggests Insys’ case may be somewhat different.
Former employees say that about 90 percent of Subsys prescriptions were for off-label uses. This happened as a prior-authorization unit executive (and her supervisor) allegedly spent the past three years developing new and improved ways for employees to gull insurers with misleading patient diagnoses and codes, as the Dec. 3 article described in detail.
With the company’s achieving market-leading prescription-approval rates of 85 percent to 90 percent, the alleged scheme of Insys’ prior-authorization unit easily cost insurers hundreds of millions of dollars. They are unlikely to write off these losses without a fight.
Moreover, federal prosecutors will seek recovery on behalf of their employer, the U.S. government. Data obtained via the Freedom of Information Act shows that nearly 25 percent of Insys’ $576.5 million in revenue for Subsys since its launch, or $144.1 million, comes from Medicare and Tricare. While not every prescription was unlawful, with a potential fine of $10,000 per violation, the ones that were could result in an eight-figure company liability.
One saving grace for Insys may be its decent cash position at the end of the third quarter, with just a tad less than $94 million in cash and equivalents available and an additional $61.5 million in short-term investments.
The graph below captures what almost four years of Insys’ selling Subsys off label across the United States looks like.
Sources: IMS Health and FDA Adverse Events Reporting System data through June 30, 2015
Here the Southern Investigative Reporting Foundation plotted IMS Health’s prescription counts for Subsys adjacent to the FDA’s Adverse Events Reporting System data listing fatalities for which Subsys was listed as the probable candidate for triggering an adverse reaction.
This FDA data is not definitive, as it relies on informal assessments by medical professionals that are voluntarily reported. (An Insys press release last week took exception to the Southern Investigative Reporting Foundation’s reporting and offered its own interpretation of what the FDA data means.)
————————
For more than nine months the Southern Investigative Reporting Foundation has documented Insys’ freewheeling, compliance-light approach to selling Fentanyl. In the course of this reporting, it became clear that Insys’ approach to building and managing its sale force was both the key to its explosive growth and its subsequent woes.
The experience of Insys salesman Tim Neely, a 43-year old former fireman from San Clemente, Calif., is illustrative of how good intentions and honest ambition can be thwarted by a company’s drive for expanding earnings at all costs.
The Southern Investigative Reporting Foundation began talking to Neely while he wrestled with the company over a bereavement leave dispute in the late summer. In October Insys fired him. He has retained a labor lawyer and, in his words, “is examining his options.” In short, Neely is by no means a neutral observer.
Nonetheless, in addition to talking on the record, Neely provided documents, texts, emails and personal notes taken during calls with managers. Anything he discussed was checked with current and former Insys sales reps and managers, several of whom also provided documents. Finally, a reporter spent four days in California and confirmed and corroborated his account.
All signs point to the fact that Neely was a very good sales rep for Insys.
Based on the value of prescriptions, he ranked within Insys’ top 15 sales representatives last year, an achievement good enough to place him in the “President’s Club,” with one perk being an all-expenses-paid Mexican beach junket with other sales leaders. This is noteworthy considering the fact that he began selling pharmaceuticals only in October 2013.
Neely told the Southern Investigative Reporting Foundation that he earned $207,000 last year and, based on the documents he provided, he was on track to earn $170,000 to $180,000 this year.
A proud daily surfer, Neely would tell beach buddies and his family in emails and texts that he had taken a lot of risk leaving the job safety and camaraderie of the firehouse for Insys but that he was doing well and felt good about helping people who were in pain.
But late last summer Neely changed his mind in a big way about Insys.
While remaining a “true believer” in Subsys’ potential as a drug (a broken back a few years ago made him an expert on breakthrough pain, he said), Neely started to become troubled about the integrity of Insys’ management.
Neely said he felt management pushed the sales force to market Subsys “to anyone with a prescription pad.” Anyone who disagreed with that approach, he said, “was treated like garbage” and eventually fired.
His customers were several veteran surgeons who prescribed Subsys with regularity. Based on Neely’s documents and notes, he did what Insys trained him to do — become nearly indispensable to his clients. He instructed patients on the proper use of the drug in doctors’ offices and worked to overcome numerous impasses between patients and insurance companies. His doctors liked him enough to regularly allow him inside their office suites if he needed to make calls to schedule other appointments.
Like many a sales rep in any field, Neely hustled to keep his doctors happy. In one case, Neely arranged the weekly rental of a Beverly Hills basketball court for a regular pickup game with a doctor and his friends; in another, he celebrated a doctor’s birthday with sushi and tickets to a Los Angeles Kings hockey game.
And plenty of prescriptions were written, so much so that Neely said he takes pride in never having asked a doctor to prescribe the drug. The prescriptions were (usually) for cancer and postoperative trauma patients, keeping him far away from legal headaches.
But, as he described it, that wasn’t good enough. Insys’ management wanted more and wished him to somehow try to persuade the doctors to move the prescribed dosage to 800 or even 1,200 micrograms, even if the patient was doing well at 400. To Neely, doing so was destined to hurt patients and strain lucrative relationships.
“Serious doctors don’t want criticism on their dosing [protocols] from a sales rep and they don’t need [Insys’] speaker program money,” Neely said. But “the crappy ones” will and do, he added. “There’s just a point where you can’t sell more Subsys without crossing some lines. It’s not a [skin care] product; it’s not like other drugs.”
Neely and other former Insys reps described the pressure to constantly land new prescribers as unrelenting. Company departures became the norm, with many seasoned pharmaceutical sales reps leaving within weeks of being hired.
The pressure to generate sales revenue often reached absurd levels, according to one former Insys sales manager who for a decade had sold pain-management drugs at other companies. He said the sales leads the company gave his representatives were culled from a database like the yellow pages and had no connection to pain management or oncology. At varying times, his reps were asked to call on a naturopathic healer, a self-described shaman, several chiropractors and a nurse midwife, none of whom were able to prescribe Fentanyl — let alone needed to, he said.
His complaints to management were ignored. After concluding that there was no real business plan, this sales manager resigned three months later.
Another distinctive feature of life at Insys, Neely said, was adapting to what he described as a form of corporate schizophrenia: “Sales training and company-wide phone calls would be by the book, exactly like Merck or someone might do. Then your [district and regional] managers would pull you aside and tell you, ‘Don’t worry about that. Just sell. Do what you need to do.'”
The “say one thing, do another” culture became apparent early on to Neely.
During his training week, after a series of discussions on Subsys’ chemistry, how it compared to rivals and its place within the transmucosal immediate release Fentanyl marketplace, Neely and his sales trainee colleagues were told they were taking a test the next day — and failure would result in dismissal. A few hours later, a regional manager emailed them the answers to the exam — and the group was taken out drinking until the early morning by sales managers.
A core part of Insys’ sales training involved discussion of the company’s policy against wining and dining prescribers. Shortly after attending that presentation, a still green Neely wound up one night with a prescribing doctor (and his troop of thirsty friends) drinking and smoking cigars at a swank Beverly Hills club. The $530 bill was handed to him straightaway and he paid.
Pharmaceutical companies now disclose what they spend on physicians, either in terms of speakers program fees, research payments or hospitality, per the Physicians Payment Sunshine Act. No record of Neely’s boozy evening has been disclosed.
A few days after his Los Angeles outing, a district sales manager, Darin Cecil, told Neely that since that doctor was a good prescriber, the company kept a credit card available to help pay for just those expenses. Cecil told Neely that this had to be done “quietly” (he was given the card number via a text message) but a sales rep could use it to order sports and concert tickets. And a sales rep could be reimbursed for other events, too. Just as long as prescriptions were written afterward, Neely was told, no one would have any problems with the practice.
Through this hidden reimbursement channel Neely expensed thousands of dollars in entertainment charges — and he was not the only one, according to his former Insys colleagues. Neely said he was led to believe that then CEO Michael Babich knew about the practice but Neely was instructed to never bring it up publicly.
Neely was reimbursed for his charges every time.
————————
While Neely might not have been aware of what other sales reps across the country were doing to sell Subsys, he readily said, “I certainly felt some of the stuff [management] said was OK to do was probably not.”
One controversial practice that Neely described was the following: Sales reps were told to seek permission from staff in doctors’ offices to go through patient files looking for likely Subsys candidates, which, depending on the circumstances, could be a violation of patient privacy standards under the Health Insurance Portability and Accountability Act.
“They treated HIPAA like it was a joke,” Neely said, describing how sales reps, managers and their assistants regularly sent one another emails discussing patients’ treatments, including their diagnoses and dosages. Neely’s files are indeed full of Subsys user data.
Insys had some reasons for that. The prior-authorization program allowed Insys access to patient data so the company could try to secure insurer payment — and the sales rep was usually the point of contact for the patients, telling them when coverage was approved, about next steps, or if coverage was declined, how to initiate an appeal.
The procedures before the weekly sales conference call in Neely’s district illustrate how Insys’ real-time data collection, when combined with the patient disclosures from the prior-authorization program, could lead to potential disclosures of personal health information, according to Neely. Prior to the start of the call, Neely’s district manager would send an email detailing a list of prescriptions that had not been renewed or picked up or that had been canceled, indexed by the prescribers’ names. The idea was that the sales rep would call the prescribers to try to work for a renewal of the prescription or reverse a cancellation.
What was unsaid was that the sales reps likely knew — or at least could take an educated guess about — the names of many of those patients from the prior-authorization process. This led to, in several instances, sales reps’ contacting the patients directly and encouraging them to ask the prescriber for another, stronger Subsys prescription.
Then there were the episodes so far outside industry norms that they appeared surreal to Nealy.
At a cocktail party during a 2014 sales retreat, according to three of the attendees, one sales manager told her colleagues about an NBA star who had been prescribed Subsys for postoperative pain. This revelation stunned those who had heard it into silence until one wag remarked, “Well at 800 micrograms for 90 days, I guess, he won’t be back for the playoffs.”
In another instance, the Southern Investigative Reporting Foundation obtained a text from a pharmacist who sought a manager’s help locating an Insys sales rep named Brook Spangler. The text described how Spangler had purportedly — and inexplicably — been given a patient’s Subsys prescription but had not dropped it off.
(Contacted for comment, Spangler denied every aspect of the story: “I have never had a patient script in my hands, ever.” When read the contents of the text, she said it was a mistake. Messages left for the pharmacist were not returned.)
————————
The Insys executive who suggested examining patient files — albeit with the permission of office staff — and the biggest proponent of using a so-called secret credit card for entertainment expenses was national sales chief Alec Burlakoff.
Burlakoff’s vision for sales reps at Insys pushed the boundaries of pharmaceutical sales. He wanted them to be so integral to the patient’s experience with Subsys that a doctor would not think of prescribing other drugs. Sales representatives who had worked under him said his rationale for searching through patient files was that it was a win-win proposition: Insys could get additional prescriptions written and the doctor could receive speakers program fees.
A man of incalculable energy and a dynamic speaker, Burlakoff has been a frequent focus of Southern Investigative Reporting Foundation reporting on Insys. His effect on new sales reps was, as Neely put it, “incredibly powerful.”
Also powerful was the effect of his sales policies upon Insys’ income statement. As Burlakoff departed in July, annual sales were anticipated to be $300 million; when he became sales manager in early 2013, the company had just reported about $16 million in revenue.
By the time Burlakoff was lecturing Neely’s late October 2013 training class on his sales views, his strategy was generating tremendous returns in the form of double- and triple-digit quarterly sales increases. So when he spoke, everyone at Insys listened.
“If you can keep [patients] on [Subsys] for four months, they’re hooked,” Burlakoff told Neely’s training group. “Then they’ll be on it for a year, maybe longer.”
(Privately Neely would ask him if by “hooked” he meant addicted. In reply, Burlakoff gave him a puzzled smile and would only say, by way if clarification, “It’s not addicted if [the patient] is in pain.”)
Like many sales managers, Burlakoff used pop cultural references to drive home his goals. In an early 2014 sales meeting that Neely attended, Burlakoff told a group of several sales reps that if they hadn’t seen the then newly released movie “The Wolf of Wall Street,” they needed to see it right away.
Burlakoff said, according to Neely, “It’s the best sales training video in history” (although carrying out its lessons could result in federal prison sentences.)
Another video that Burlakoff found inspiring was something he showed Neely toward the end of his training week. In a break after a session, Neely was pulled aside and shown a video of a man using a dildo to pleasure a woman. After the smartphone-shot clip ended, Neely found himself speechless.
“Alec,” he said, “what’s that about?”
To which, Neely said, Burlakoff only smiled and walked away.
Burlakoff had a very specific vision about the people he wanted at Insys.
For instance, Burlakoff rejected the framework of hiring and training practices of what he derisively called “Big Pharma.” He preferred to hire salespeople who were used to the pressure of having to make quota or face dismissal; prestigious colleges weren’t very important for that skill set. A sales rep who needed to get three prescriptions written in four days (or else) would push Subsys without dwelling on too many other things.
Because all that Burlakoff valued was sales — generating prescriptions — he made rather unusual hiring choices.
In April, for instance, the Southern Investigative Reporting Foundation reported on his decision to hire Sunrise Lee and make her sales chief of the Midwest region. They had known each other when Lee worked as a stripper in Miami and apparent escort agency owner. Lee’s Insys job centered largely 0n socializing with prescribers. Burlakoff described Lee’s professional skill in serving as “more of a ‘closer.'”
Burlakoff hired numerous women for key sales roles. As is the case at many pharmaceutical companies, the women were uniformly attractive and several had unique backgrounds. There was Amanda Corey Emhof, a former reality-TV show star who had won $477 on an episode of “Judge Judy” and had once considered becoming a sex therapist.
Prior to selling Fentanyl, Emhof posed for Playboy [NSFW]. She co-founded Thrive Model Management, a business that provided models for marketing campaigns and private parties where she heads “model managing.” Reached on her cell phone the day before Thanksgiving, she declined to comment.
Insys’ apparent practices of hiring women based on their looks, with extraordinary economic incentives to sell the drug, resulted in a good deal of extracurricular sales rep-doctor relationships complicated by sex. None more so than in 2013 when the wife of a high-volume Subsys prescriber found a revealing photograph of an Insys sales executive on his phone. Since she lived not far from headquarters, she drove there and raised a ruckus; she was assured that all appropriate measures would be taken against the rep.
The sales rep was promoted soon after to sales trainer; the doctor no longer prescribes much Subsys.
While Burlakoff’s laissez faire sales approach led to a great deal of revenue, some take issue with its practices. Dr. Ken Bradley, a Torrance, California-based pain management physician, said that he disagreed with Insys’ sales approach.
“Not a lot of doctors are going to write a [prescription for a drug] whose rep doesn’t understand it very much and dangling speaker programs in front of them doesn’t make up for that,” Bradley said, referring briefly to a sales rep he had dealt with who had worked in auto leasing before joining Insys.
Bradley added that he had, upon joining a practice, “inherited several patients” using Subsys but that after their course of treatment was completed, he declined to further prescribe the drug. (To be fair, he said the drug worked as it was supposed to.)
“The high-pressure sales tactics became annoying and were just another reason to not deal with [Insys’] sales staff,” he said.
Dr. Bart Gatz, a Boynton Beach, Florida-based pain-management doctor with multiple offices, said that the regulatory and insurance headaches associated with prescribing Subsys have “made it impossible to prescribe.” He added that he didn’t think he had written five prescriptions for the drug this year.
Coming from him, that’s devastating news for Insys: Gatz was the sixth leading prescriber of Subsys under Medicare in 2013 and was Insys’ fourth highest recipient of speakers program fees in 2013 and 2014, collecting more than $154,000.
“I’ve seen this a few times before where a company just grows too fast and does stupid things, gets some doctors to write inappropriately and the feds come down all over them and everybody else,” Gatz said. “That’s what happened here. It’s over.”
Gatz added that he liked Subsys and that it worked well for patients who couldn’t swallow or digest easily during chemotherapy regimens, but authorizing insurer payments had proved so difficult this year that he had switched his patients off the drug.
Asked about his Insys sales representative, Gatz mentioned that “she hadn’t been coming around very much” since he stopped writing prescriptions for Subsys. He said that it was difficult beginning a dialogue with her about Fentanyl products given that her previous job had been working as a cashier at a Publix supermarket.
————————
Everyone named in this story was contacted for comment by phone, email and, if possible, text message — often multiple times.
Except where noted, no replies were received.
In all cases detailed messages were left about the nature of the Southern Investigative Reporting Foundation’s inquiry.
Insys Therapeutics, despite its profitability and current high profile, is unique in that it doesn’t have either an internal media relations staff nor an external advisor.
Calls seeking comment were directed to chief financial officer Darryl Baker, who did not return a call and text message sent to his cell phone.
Insys Therapeutics is a company in a great deal of trouble.
The manufacturer of a Fentanyl spray called Subsys with 100 times the strength of morphine, Chandler, Arizona-based Insys scored the top-performing initial public offering of 2013, according to CNBC. Analysts and investors adored the company’s fast sales and profit growth and dreamed of a future when Insys’ cash flow would lead to dividends and acquisitions.
As Insys’ market capitalization topped $3 billion, those who got in on the ground floor, investing early on, shared in its success: Founder Dr. John Kapoor became a billionaire and a host of company insiders, led by CEO Michael Babich, became millionaires.
Their joy was not to last.
Starting late last year critical press reports detailed alleged business practices at Insys so aggressive as to make the company an outlier in the oft-sanctioned pharmaceutical industry.
It wasn’t long before subpoenas began to pile up, with state and federal prosecutors on both coasts swinging into action; the U.S. attorney’s office in Boston, for example, impaneled a grand jury (and grand juries rarely fail to return indictments). Indictments of Insys’ most frequent prescribers continued and key executives have departed without notice.
Then came the lawyers.
In August, Oregon’s Department of Justice arrived at a $1.1 million settlement with Insys that represented about twice the amount of its revenue in that state. (In April, the company had settled a class action for $6.125 million.)
The proposed resolution from the Oregon Department of Justice makes for stark reading; it uses depositions and emails to claim that the company misrepresented a key scientific study, encouraged off-label prescriptions (allegedly in violation of U.S. Food and Drug Administration guidelines) and ran its speakers program solely to reward frequent prescribers.
While Insys’ investors haven’t thrown in the towel (the company’s share price has risen a split-adjusted 50 percent in the past year, in some measure because Kapoor and his family’s trusts control 66 percent of the outstanding shares), investor enthusiasm is starting to wane.
On Nov. 2, on the eve of an earnings announcement, CEO Babich suddenly resigned — a move that typically raises a major red flag for investors. Kapoor, who assumed the CEO mantle, told those listening on the conference call, “Mike decided that now is the best time to turn the page and focus on his family as well as pursue new opportunities.”
There’s more to the story, though.
Babich was forced out by Kapoor, according to a senior Insys executive who was in regular contact with Kapoor in the days prior to the announcement. While both men are the subjects of intense regulatory scrutiny, the founder and chairman bluntly told his lieutenant of 14 years that Babich was closest to the issues that federal prosecutors were looking at and that a change had to be made should settlement talks became serious, according to the executive source.
While Babich may be spending time with his young family, his personal life is more complex.
Earlier this year, Babich began a relationship with Natalie Levine, then a Boston area Insys sales executive who subsequently became pregnant; they married in the summer. (This is Babich’s second romance with a sales colleague; Kapoor has also dated two sales executives.) Aside from the fact that it’s unusual for a public company CEO to date someone who reports to him, the Babich-Levine relationship had another dynamic to it.
The newlyweds will probably be monitoring the developments in a rapidly expanding criminal suit filed in the U.S. District Court in Hartford where Heather Alfonso, an advanced practice registered nurse who was a high-volume Subsys prescriber over the past two years, pleaded guilty to accepting $83,000 in kickbacks. Federal prosecutors, according to the transcript of the July plea hearing, allege that the kickbacks prompted her to write Subsys prescriptions worth $1.6 million.
What appears to have brought the federal prosecutors’ intense scrutiny of the divorced mother of four was the baldness of the scheme. According to her plea, Alfonso was paid $1,000 each time she attended an Insys speakers event, where she was supposed to discuss with other medical professionals her clinical experience of Subsys. In reality, however, no other prescribers were present, and prosecutors said the events amounted to nothing more than Insys-sponsored dinners and drinks for Alfonso and her co-workers.
Natalie Levine was one of the sales staffers who called on Alfonso, and Levine arranged and attended many of the 70 speakers program events. As CEO, Babich approved two years’ worth of budgeted payments to Alfonso.
(While courts have traditionally recognized spousal privilege and declined to compel a husband or wife to provide testimony about a spouse, the events in the Alfonso case occurred before Levine and Babich married.)
Alfonso is cooperating with the government, as might be expected for someone facing a possible sentence of 46 to 57 months in jail; her sentencing date has been pushed back twice, most recently for six months. In the plea hearing transcript, prosecutors offered a pretty big clue about where Alfonso’s cooperation might be taking the investigation. For example, several Medicare Part D beneficiaries were described by prosecutors as ready to testify that she diagnosed them with having issues other than breakthrough cancer pain (the primary condition Subsys is indicated to treat) yet insurers still authorized the prescriptions.
As described in the transcript, Insys’ prior-authorization unit changed Alfonso’s diagnoses to cancer. Absent the alleged changes, the prosecutor asserted, the insurers would have never paid for the prescriptions.
And as the Southern Investigative Reporting Foundation wrote in July, Medicare and commercial insurers appear to have approved reimbursement of prescriptions for Subsys at vastly higher rates than those of its rivals in the Fentanyl marketplace.
The prior-authorization unit was set up to assist patients with complex insurance paperwork. Its value proposition was simple: The patient signs a few forms and Insys handles the messy paperwork. Patients would get the medicine, prescribers wouldn’t have to scramble for an alternate medication and Insys would book thousands of dollars in revenue per prescription.
In reality what the prior-authorization unit did was take advantage of pharmacy-benefit manager inertia to work a type of bureaucratic alchemy, whereby a torrent of off-label Subsys prescriptions would be transformed into ones associated with medically urgent cancer diagnoses.
Unmistakably, the prior-authorization unit was the key piece in helping Insys double the size of the Fentanyl marketplace to more than $500 million in less than two years.
Lost in the cascade of prescriptions, however, is the human toll from peddling Subsys like a new piece of software or an improved detergent. Since the drug was launched in January 2012, the FDA’s Adverse Events Reporting System lists 203 deaths for which medical providers have fingered Subsys as the probable candidate for triggering an adverse reaction. Moreover, the pace of purported Subsys-related deaths has been accelerating, with the FDA’s disclosing 52 deaths in the second quarter of this year alone.
(This FDA data is not definitive: It relies on voluntary medical-provider reporting so the number of incidents may be undercounted. Additionally, most reports represent a medical professional’s assessment and do not present an official cause of death.)
These deaths have occurred amid a nationwide opioid abuse epidemic. According to the Centers for Disease Control, in 2013 (the most recent year for which data is available), 16,235 Americans died from prescription opioid overdose. Subsys is now the top-ranked “diversion drug of concern”or the most frequently stolen or fraudulently obtained, according to the Department of Health and Human Services’ Office of the Inspector General.
What follows below is a description of what happens to a company when rule bending is institutionalized and the pressure to make a sale has deadly repercussions.
————————
Danielle Gardner worked in Insys’ prior-authorization unit for a year and feels terrible about it. She is convinced that the unit’s arranging for insurance company approvals for thousands of off-label Subsys prescriptions led to the addiction or death of a certain percentage of the patients involved.
Gardner, whose name is a pseudonym, would love to be told that she’s jumping to conclusions, that there’s no concrete proof of anything like that. But the plain fact of the matter is that she is almost certainly right.
For a portion of her professional life, Gardner woke up each day to perform a job with a singular goal: to do anything to make the employees who handled pharmacy benefits for insurers think that the people who had been prescribed Subsys had cancer when only 1 percent of them did.
She and her seven or so colleagues did that one thing very well and many people made a great deal of money.
Gardner began her odyssey at the prior-authorization unit after her application submitted via a job-hunting site led to an interview. During her visit to Insys’ office, she deemed its operations to be busy and serious. To her, Insys seemed to be a growing company whose only business, as she was told, was helping people beat cancer.
“I liked the idea of helping people with the paperwork, which can be the hardest part of health care, but mostly I needed a job and [$18 to $20] per hour and benefits” was very good for Phoenix, she said. Better still, there was the prospect of bonuses. A veteran of several doctor’s offices, Gardner was well versed in obtaining insurance company approvals but had never heard of employees in a prior-authorization unit receiving bonuses. The decision was “yes” or a “no” proposition. How money came into the equation baffled her.
But her co-workers swore they were receiving the bonuses.
The bonus wasn’t the only matter that Gardner had questions about, though. She didn’t know why Insys’ prior-authorization unit was located across the street from headquarters or why the lobby had no sign for the division. The unit had a different phone exchange and a separate email server.
But Gardner kept her mouth shut.
While her boss Liz Gurrieri who ran the prior-authorization unit could be friendly, she had made very clear to everyone that the best questions were about how to do the job better. Gurrieri had built the unit from the ground up in 2012 and was held in the highest esteem at headquarters. In just a few years, as the story around the cubicles went, Gurrieri’s stock options had helped her become wealthy enough to build a six-bedroom house.
So everyone in the unit did things Gurrieri’s way because the money was good.
After a brief training period, Gardner went to work. Each day Gurrieri handed out stacks with five patient charts to Gardner and her seven colleagues and they would dive right in to make calls.
Prior-authorization unit staffers had a very specific formula that governed their life. Individually they had to secure 25 Subsys approvals a week; during a Monday meeting, Gurrieri’s boss, Michael Gurry from the corporate office, would tell the prior-authorization team the “group gate,” or minimum number of total approvals expected for the week, usually at least 200.
Assuming that the minimum was met, for every additional approval Insys gave $7 to a “bonus pool.” For example, if the prior-authorization unit received 300 approvals, then the bonus pool was $700 per person.
Plus there were individual bonuses: After a prior-authorization staffer secured 35 approvals, Insys gave the employee a $50 bonus and $10 for each incremental approval. So if Gardner received 47 approvals for the week, she would earn an extra $170 bonus on top of the $700 pool-based bonus. (A team member who failed to hit 25 was not eligible for a bonus.)
In a good week, Gardner found she could arrange for as many as 55 approvals; others achieved even more. After taxes, she was bringing home $3,000 to $3,500 a paycheck.
All she had to do, of course, was to change in the charts the insurance codes for the diagnosis of back or joint pain, organ problems, work accidents, military trauma or menstrual cramps into cancer ones.
Until the subpoena from the Department of Health and Human Services’ Office of Inspector General arrived at the end of 2013, that proved to be easy for her.
Up to that point Gardner would reply yes to pharmacy benefit manager employees who asked if the patient had “breakthrough cancer pain,” Gardner said. Then it was a slam dunk. Very few insurers wanted to be accountable for denying a cancer patient pain medicine. No matter what else changed, confirming a cancer diagnosis remained a requirement for any patient whose doctor was prescribing him or her Subsys for the first time, Gardner said.
Everything had been scripted per instructions from Gurrieri, with each phone call beginning with an identification of the prior-authorization unit staffer as being “from Dr. ____’s office.”
No one argued with success as the prior-authorization unit’s approval rates ran as high as 80 percent or more. They were limited only by the number of prescriptions written.
Despite the sharply increasing volume of Subsys prescriptions by the start of 2014, few, if any, pharmacy benefit managers had linked the prior-authorization unit to Insys.
Then again, few details were overlooked in keeping the connection obscured.
Outgoing phone numbers were blocked to avoid showing up on a caller ID and staffers were under orders to never use the company’s name when speaking to anyone from an insurer or a pharmacy benefit manager; if pressed, they would only say that they “were working closely with Dr. ___’s office.” When providing a phone number for a return call was required, they gave out a toll-free 800 number that would be answered by a colleague named Shannon. She would quickly direct the caller to the prior-authorization staffer without fielding any questions.
After the arrival of the Health and Human Services subpoena, which Gurry assured the prior-authorization unit staff was just a routine federal inquiry that a certain number of pharmaceutical companies underwent every year, Gurrieri ordered a change of strategy, Gardner said.
Instead of answering yes to questions about breakthrough cancer pain, prior-authorization unit staffers were to answer, “yes, they have breakthrough pain,” which was both an affirmative answer but ambiguous enough to mean virtually anything. Plus, pharmacy benefit management call-center employees, some of whom were located overseas and with hourly or daily quotas for handling calls, might mishear one or two words and consider the question properly answered. (The prior authorization unit never discussed the fact that insurers may have been given a false impression, according to Gardner.)
Through the spring of 2014, approval rates remained impressive, but pharmacy benefit managers began to push back, sometimes demanding to speak with the physician about the diagnosis. If the pharmacy benefit manager called the prescriber, that was a big problem in and of itself as the prior-authorization unit was in no way “from” any doctor’s office.
Messy episodes sometimes occurred, Gardner said, with physicians angrily insisting that no one by the prior-authorization staffer’s name worked at their office and that the patient in question did not have cancer.
Gardner said there were rarely long-term issues with pharmacy benefit managers, who would usually accept the prior-authorization unit’s explanations of misread charts and human error as an explanation. Doctors, too, often accepted an apology from the sales rep or a district manager.
By mid-2014, the fortunes of prior-authorization staffers were changing. The subpoena that Michael Gurry had assured them was part of a standard procedure for pharmaceutical companies didn’t go away and another arrived after Labor Day.
Given the legal issues that several key Subsys prescribers were experiencing, Gurrieri ordered Gardner and her colleagues to begin phone conversations by referencing “calling on behalf of Dr. ______’s office.”
Even so, approval levels were dropping in the late summer of 2014 as pharmacy benefit managers began demanding more detailed answers about diagnoses for a Fentanyl prescription. The approval woes went unnoticed to the world, however, as a spike in newly hired sales reps kept the prescriptions rolling in.
To reverse the trend of a slowdown in number of approvals, Gurrieri developed what prior-authorization staffers called “the spiel,” a series of dialogues (to commit to memory), designed to address detailed questions about whether a patient had breakthrough pain and cancer.
When someone from a pharmacy benefit management office asked about a patient’s having breakthrough pain from cancer, the prior-authorization staffer would reply, “The physician has stated that Subsys is approved for treating breakthrough cancer pain so (he or she) is treating breakthrough pain.”
While this response was wrestled with, prior-authorization staffers, per their instructions, would invent conversation to suggest they were right inside the prescriber’s office — something along the lines of “You should see this guy. It’s a real sad case and the doctor is upset about it.”
Approval rates began to stabilize and even inch back up, yet some of the biggest insurers began to become strident in their refusal to approve Subsys. Gardner said she told Guerrieri this, who pulled her into her office and instructed her to change the insurance code on patients charts to 787.20 on the most difficult cases. That was the code for dysphagia, a condition of having difficulty swallowing that’s related to illness. This served to box in the pharmacy benefit manager because a denial of a Subsys prescription could run the risk of starving a patient. This technique worked every time to secure an approval.
In addition, Gardner was ordered to intentionally mix up insurance codes, to substitute in, say, 338.30, associated with cancer-related chronic pain, for 338.29, which is for general chronic pain not connected to cancer.
Shortly after that, though, in the autumn of 2014, Gardner began to suffer anxiety related to performing what she was certain constituted unethical behavior, she said. She left the company shortly afterward.
“I couldn’t take [the misrepresentation] anymore,” she said, adding that she was “traumatized by thoughts of getting arrested.”
Gardner told the Southern Investigative Reporting Foundation that she had cooperated “extensively” with federal law enforcement officials over the past year about the nature of her prior-authorization job at Insys but declined to say she was asked about.
Her description of events at Insys’ prior-authorization unit was corroborated by other Insys employees, including sales representatives and managers, who had frequent contact with the group, a physician who was familiar with its operations, another prior-authorization unit employee — and a description in the now-settled class action.
————————
As is the case for all Southern Investigative Reporting Foundation articles, numerous attempts were made to reach all the people in this story and provide them with an opportunity to comment on what had been reported about them. In cases where an email address was unavailable, a detailed voice message was left with questions. Over the course of several months, five attempts were made to contact Michael Babich and Natalie Levine on their mobile phones by leaving detailed voice messages and sending texts. They did not respond.
A call to Insys was referred to the company’s chief financial officer, Darryl Baker, and a voice mail was left on his office phone. A later call was placed and a message was left on his mobile phone as well. He never responded.
Michael Gurry did not reply to a voice message left on his office phone.
Multiple attempts to seek comment from Elizabeth Gurrieri were made that included messages being left on her cell phone and texts. On the one occasion she answered, she declined to comment, citing time constraints.
Poland seems a most unlikely place for the next chapter of Valeant Pharmaceuticals’ saga to play out. Weighing in with about 3 percent of sales, the Polish operations are seemingly a modest contributor to Valeant’s fast-growing bottom line.
But Valeant’s Eastern European operations have recently been the source of a good deal of message board rumor, which in turn has prompted the company to quickly respond.
So the Southern Investigative Reporting Foundation set out to see whether Valeant’s units in Eastern Europe are as robust as their North American brethren. The foundation chose Poland to start with because it’s the third largest geographic segment and, along with Russia, a core component of the company’s emerging markets unit (which represented 25 percent of sales last year). Just as important, unlike Russia, Poland doesn’t have a rich civic tradition of killing investigative reporters or the people working with them.
There’s a lot more inventory in the corporate supply chain than meets the eye, and that’s rarely a good thing, at least in the long term. Moreover, this is occurring against the backdrop of a flat sales trend in Poland.
Given the complex Valeant Europe organizational chart, sussing this out wasn’t a walk in the park.
On Nov. 10, Valeant’s chief executive officer, J. Michael Pearson, during a conference call, noted that Polish inventory levels were currently equivalent to four months’ worth of his company’s then average sales rate and were slated to be lowered. The call to discuss Valeant’s business came in the wake of its Philidor-driven controversies stories that the Southern Investigative Reporting Foundation’s readers will recall it was the first to report.
Translated from business speak, what Pearson meant is that Valeant’s Polish operations has sold four months’ worth of inventory to a series of distributors, who, in turn, will deliver the products to retailers. Most CEOs want to avoid having inventory levels spike in distribution channels because over time excess supply reduces demand, which in turn forces production cuts and ultimately lowers the price of the product. (See what Valeant said when the Southern Investigative Reporting Foundation asked it about Polish inventory issues.)
But the full picture is much more complicated than that.
In Poland, three of Valeant’s subsidiaries, ICN Polfa S.A., PF Jelfa and Valeant SP. Z O, account for 98 percent of its revenue. Of the three, Valeant SP is by far the largest, amounting to about 75 percent of the revenue. It’s not, as might be expected, a manufacturer but a wholesaler, buying drugs Valeant produces in Poland and elsewhere, and then selling it to other distributors.
While Valeant’s explosive revenue growth is what made the company so beloved of investors, that hasn’t made it to Poland yet. Through the third-quarter revenue from the three units, as measured by IMS Health data, was just under $187 million and on pace to slightly improve upon last year’s $270.3 million. In turn, 2014’s sales were off relative to $296.4 million in 2013.
According to filings, at the end of last year, the three subsidiaries had 95 days’ worth of sales in inventory on its balance sheet. (There’s not a hard and fast rule for determining how much inventory is too much, but when it’s just sitting on a balance sheet and not moving, it’s a safe bet that the higher the figure goes, the more management and investors should worry.)
Add that to the 120 days of sales that Valeant recently acknowledged having in the channel. That’s 215 days of Valeant’s production chain that hasn’t made it to the retail market. Since the end of 2013, IMS Health data shows Valeant’s inventory in the distribution channel increasing to four months’ worth of sales from under two months.
To answer the question of whether that’s standard or not, take a look at how much inventory other major pharmaceutical wholesalers keep on their balance sheet. The three companies below, Neuca, Pelion and Farmacol, control nearly 70 percent of the Polish wholesale pharmaceutical market:
So Valeant in Poland is clearly moving inventory less rapidly than its peers and per above, has put additional product into the channel earlier this year given the increase to four months of sales. To be fair, the comparisons are not exact given that the other three companies are purely wholesalers and Valeant has manufacturing operations.
A spokeswoman for Valeant, Renee Soto of Sard, Verbinnen & Co., said Polish inventory levels as of yesterday were back to three months’ worth of sales.
The supply chain process in Poland for getting a drug to a pharmacy from the plant is fairly described as labyrinth. Evidence the first is an occasional fourth step in the supply chain process called pre-wholesale warehouses, which are owned by the wholesalers but aren’t tracked by IMS Health. This inventory essentially falls “off the grid” and it’s nearly impossible to see how much is in there or how long it stays.
Industry insiders in Poland say that pre-wholesale warehouses hold inventory from manufacturers and charge them between 1.2 percent to 2 percent of the value of the inventory per month as a fee.
Then there is Myslowice, a 138,000-square-foot warehouse located equidistant between Valeant’s two other facilities in Jelenia Gora (546,000 square feet) and Rzeszow (412,000 square feet). One cannot easily find the facility listed on the company’s website because it leases it from DHL, the giant shipping and logistics company whose Exel unit often leases properties to work with key clients.
A recently granted license allows it to operate as a pharmaceutical wholesaler but unlike the other two facilities its permit allows it to sell on consignment. While consignment sales are fully legal, from an accounting perspective they often raise earnings-quality questions. (Bausch & Lomb, then an independent company, was ensnared in a consignment sale scandal in the 1990s.)
Valeant says the facility is currently its main distribution hub for Poland and Eastern Europe and that it does a small amount — about $4 million — of consignment sales there for a hospital unit. Read its full response.
On Valeant Pharmaceuticals’ conference call on Nov. 10, embattled chief executive J. Michael Pearson offered several defenses of his company’s internal controls and procedures.
Similarly, in defending both himself and Valeant from the now constant drumbeat of controversy, one of Pearson’s constant refrains has emphasized his commitment to transparency.
A March 11, 2014, Securities and Exchange Commission filing suggests Pearson and Valeant have a long way to go on both of these fronts. Put bluntly, a footnote in a Valeant filing more than 18 months old appears to show how Pearson made a handsome profit through what is referred to as an unspecified “error.”
How handsome? Thanks to a rocketing stock price and corporate opacity, Pearson picked up a block of stock for $20 million less than it was then worth.
(Southern Investigative Reporting Foundation readers will recall its Oct. 19 revelation of the company’s secretive relationship with Philidor, its captive — and soon-to-be shuttered — specialty pharmacy that kicked off this trauma for Valeant. On Oct. 25 a follow-up story was released.)
Let’s start with why this is a truly unusual document for a Form 4, an often ignored class of company filings that disclose corporate insider share purchases and sales. Traditionally, the value of Form 4’s are usually interpreted in connection to a broader context or event, like executives selling into a potential corporate share repurchase or their buying shares because of an improving sales outlook.
In this case, given the unusually heavy weighting Pearson’s compensation plan has toward share price appreciation, a March 2014 Form 4 filing noting his acquisition of 502,996 restricted stock units — shares awarded only when share price appreciation triggers are met — was to be expected given Valeant’s then soaring stock price.
But then take a look at the filing’s footnote No. 2: “On May 24, 2013, the Registrant delivered 502,996 vested performance share units (the ‘2010 PSU Grant’) to Mr. Pearson in error. In connection with Mr. Pearson returning to the Registrant the value of such shares on the date of delivery (plus interest), Mr. Pearson has been credited with 502,996 vested share units to be delivered to him in accordance with the terms of the original 2010 PSU Grant.”
The awarding of 502,996 shares to Pearson “in error” is difficult to imagine for anyone who understands the compartmentalization of a large company.
Valeant is a large, fully-staffed corporation and Pearson’s compensation is closely scrutinized by both its board of directors and lawyers. As such, any clerical error would likely have been immediately caught.
Notwithstanding the error, there is no filing detailing the initial grant. The only mention of the block prior to March 2014 is found buried in a footnote on page 32 of Valeant’s 2013 Proxy noting that the 502,996 RSUs had met their vesting triggers. Previous RSU grants, especially one for 486,114 shares in 2011, don’t seem to have generated any problems.
What we can say is that this is the kind of mistake that happens all too rarely in the professional lives of most people. On May 24, 2013, the date of the initial–and errant–restricted unit award Valeant’s share price was $84.47; on March 11, 2014, the stock closed at $139.96, a difference of $55.49. According to the footnote, Pearson appears to have rectified the error by writing a check for the “value of such shares on the date of delivery.”
The footnote’s language suggests that “the date of delivery” is May 24, 2013, meaning that sometime before March 13, 2014 — the date of the Form 4’s filing with the SEC –Pearson wrote a check for about $42.48 million (plus an unspecified interest rate) to own a block of Valeant shares that was then worth over $70.39 million, a nearly $28 million differential.
It’s not clear if these shares were part of the block of 1.3 million shares (out of 2 million originally) that Pearson had pledged to Goldman Sachs for a $100 million personal loan. The shares were seized by Goldman last week when he was unable to make an October 30 margin call.
The Southern Investigative Reporting Foundation requested comment from Valeant through Renee Soto at Sard Verbinnen, its outside public relations adviser. She said the company would not comment beyond its previously made disclosures. A follow up phone call was not returned.
The Southern Investigative Reporting Foundation’s story looking at Valeant Pharmaceuticals’ well-concealed relationship with Philidor Rx Services, struck a nerve.
Briefly, the story explored the ways in which Philidor, a specialty pharmacy whose sole customer is Valeant, used opacity and some misdirection to try and build a national pharmacy network. Additionally, the Southern Investigative Reporting Foundation uncovered how Valeant had sought to conceal its control of Philidor.
A Valeant conference call scheduled for Monday morning, Oct. 26 is designed to explain these previously hidden relationships and, more importantly, calm the very frayed nerves of its battered shareholders.
But recently uncovered documents from a litigation between Philidor and R&O Pharmacy are probably going to have the opposite effect, in that they illuminate what can only be described as a bizarre effort to circumvent California regulations. Moreover, R&O’s allegations have been known to Valeant management for a month.
Additional Southern Investigative Reporting Foundation reporting has revealed that Valeant has been closely involved with Philidor at every stage of its life cycle, controlling it in all but name, since day one.
This pain isn’t being borne for no reason, however. The foundation’s reporting indicates that Philidor is almost certainly one of the most important parts of Valeant’s business.
————————
On July 21 Russell Reitz, a 64-year-old pharmacist and the “R” in R & O Pharmacy, was working in his office when a visitor dropped in unannounced. It was Eric Rice, an executive with Isolani, the company that had struck, what he thought, was a deal to buy the small compounding pharmacy back in December.
Rice had flown in from Philadelphia with several of the ranking executives of Philidor Rx Services. This Reitz found odd since when he questioned Rice about it, he insisted he worked for Isolani.
It was a tense but professional meeting and both sides left it unfulfilled.
Eric Rice was unable to come to an agreement over securing $3 million in payments he felt were due his enterprise. Reitz, for his part, had a startlingly basic question that Rice had not satisfactorily answered, both in a series of emails, and in person.
Reitz wanted to clear up once and for all, why despite his insistence that he worked for Isolani, he was always professionally connected to someone from Philidor. What was the difference between the two companies, or were they one and the same?
Rice’s colleagues, Philidor CEO Andy Davenport, general counsel Gretchen Wisehart and controller Jamie Fleming, were to Reitz’s eyes, in the middle of everything Isolani did.
Rice, whose LinkedIn profile left little doubt about where he worked, still couldn’t answer to Reitz’s satisfaction why, if he had agreed to sell his company to Isolani LLC, was Philidor the entity he always had to deal with? And what was Philidor’s real agenda anyway?
Moreover, neither Rice nor his colleagues, whose emails to him were getting increasingly strident, had ever answered another question Reitz had posed: Where was Isolani’s pharmacy permit? That they obtain their own, and not rely on R&O’s was a core component of the sale agreement. (It does not appear they ever applied for one.)
To Reitz, the huge volume of Philidor’s prescription drug sales, using R&O’s National Council for Prescription Drug Programs number, was infuriating; that a good deal of the millions of dollars in volume were in states where R&O had no registration to operate in, with drugs he never had dispensed, and filled by a pharmacy he did not own, was nauseating. To pile insult upon injury, he had refused to sign the pharmacy’s audit only to learn it was signed by Eric Rice.
This dispute had transcended the “he said-she said” realm of most business disputes a few weeks prior and was something Reitz hadn’t supposed existed apart from movies featuring the mafia taking over a business. Apart from Ray Liotta and Joe Pesci’s absence from this drama, it was in every sense a bust out.
Not that there weren’t signs that R&O was more to Isolani than just a platform for compound pharmaceutical sales. Back in mid-December, shortly after the deal was inked, Reitz was surprised to see Jamie Fleming, Isolani’s controller, show up at his office with boxes of inventory. He had a man with him who introduced himself as Gary Tanner, and who was clearly in charge. It all seemed on the up and up, if a bit sudden.
After meeting Tanner, Reitz went back and looked him up. He couldn’t understand what Gary Tanner, a specialty pharmacy expert with Valeant’s Medicis Pharmaceuticals unit was doing involved with R&O. In July, Tanner’s signing of an employment contract was something the company would later find it important enough to disclose to investors.
Reitz couldn’t have possibly known that a few months prior to approaching R&O, Philidor executive Sheri Leon had signed a California State Board of Pharmacy Change of Permit request for West Wilshire Pharmacy, despite providing inaccurate answers to standard questions. Under oath, she answered “no” to questions asking if she had ever worked for an entity that had been denied a California permit, and if any other entity owned more than 10 percent of her company.
That May, Philidor had been denied a nonresident pharmacy permit and like Isolani, it controlled Lucena Holding LLC, the entity used to buy West Wilshire Pharmacy.
On Jan. 7 Eric Rice would sign a similar document seeking transfer of R&O’s license to Isolani.
Something Reitz might have looked into, was the origin of the word Isolani. It comes from the world of chess. To simplify a complex theory, it centers around isolating the pawn, the weakest and least consequential figure in the game.
Given Reitz’s refusal to pay, Isolani sued him in September to obtain a judicial order to preserve what it alleged was at least $15 million out of a total of $19.3 million worth of checks written to it. In response, his lawyer Gary Jay Kaufman filed a 68-page declaration. The next court date is set for the middle of December.
————————
What Gary Tanner was doing at R&O was his job, which includes being the overseer, for want of a better term, of Philidor and its network of affiliated (or captive) pharmacies. Tanner’s exact title is unclear but an ex-Medicis executive said that he is Valeant chief executive Michael Pearson’s primary contact about Philidor’s operations.
This source said that Tanner has often worked in conjunction with a lawyer, Michael Dean Griffen, and another (now apparently former) Medicis employee, Bill Pickron, to source these types of pharmacy transactions for Medicis and Valeant.
The Southern Investigative Reporting Foundation’s reporting suggests that there is little to separate Valeant and Philidor beyond corporate wordsmithing. Indeed, former Philidor employees said Valeant’s executives were such a constant presence at the Hatboro, Pennsylvania, headquarters facility, that it was commonly supposed they had a block of rooms permanently reserved at local hotels.
Consider Philidor’s launch in June 2013. It’s a safe bet that Valeant heavily underwrote or otherwise subsidized the company given the long lead times of insurance reimbursement, coupled with the stress on working capital of starting a business with rapid expansion plans.
According to former employees, Philidor places heavy productivity demands on its call-center and data-entry personnel, but pays them decently: SIRF found most employees earned between $20 to $25 per hour, but in return a near 60-hour week was mandatory.
This is where the stress on working capital management factors in, since overtime would add at least $400 extra per employee paycheck. On top of that, from a late 2013 headcount of 250, Philidor added an average of 100 employees per quarter, as well as a 28,000-square-foot lease, utilities, health care, insurance and the frequent “extras,” like free lunches and coffee, to incentivize employees to stay at their workstations.
Eventually, of course, the reimbursements for the thousands of prescriptions roll in, but until then those bills have to be paid. Nothing about the economic profiles of Philidor’s management group suggests they have the ability to personally absorb the millions of dollars it cost each month to get the company off the ground.
For example, Philidor chief executive Andy Davenport, while the owner of a five bedroom, 3,500-square-foot house in nearby Horsham, has had a series of municipal liens placed against him for unpaid county and state property taxes.
————————
At bottom, pharmacies like R&O were a way for Philidor to surmount the very big hurdle resulting from the California Board of Pharmacy rejection, in May 2014.
(It is quite a read, referring to several “false statements of fact” by Matthew Davenport –the CEO’s brother — including the nondisclosure of Philidor’s true owners and their real equity stakes.)
The headache existed because, as ex-Philidor employee Taylor Geohagan put it when interviewed last week, “Billing from a [pharmacy’s] license in one state, but shipping from a California location, is against the rules.”
He would add, “Pretty much everything we did in the [Philidor] Ajudication department was use the [National Provider Identifier] codes from the pharmacies we bought out to get something [approved] in a pinch.” He described his Philidor experience in a website posting at PissedConsumer.com that said that paper copies of the NPI numbers of “sister pharmacies” were rarely handed out, and if they were, they were soon taken away and shredded.
Geohagan said that when he left the company in late summer, the practice of using multiple NPI numbers had stopped. (At least part of his animus toward the company, he wrote, resulted from resigning with two weeks of notice and being fired the next day.)
The Philidor billing department manual actually has a page that discusses using the NPIs of these so-called captive pharmacies called “Our Back Door Approaches,” according to another former employee. For example, when attempting to secure approval for a prescription with an insurance company Philidor did not have a relationship with, employees were instructed to use West Wilshire’s NPI.
Two ex-Philidor employees from the adjudication and billing departments told the Southern Investigative Reporting Foundation that the volume of prescriptions flowing into the company was massive, with billing unit workers expected to process at least 100 prescriptions daily. The former adjudication unit employee showed the Southern Investigative Reporting Foundation internal documents from November trumpeting the fact that 22,299 prescriptions were filled in the prior week. Additional documents showed other weeks that came in above 23,000.
————————
A strategic distancing from the controversial unit does not appear to be an option for Valeant.
The Isolani v. Reitz litigation reveals that Philidor’s use of these captive pharmacies is a vital revenue stream for Valeant. Some digging around in its corporate filings shows that R&O, at least before Russell Reitz began to object in July, was poised to a material contributor to organic growth.
A brief aside: organic growth, or the increase in sales apart from Valeant’s acquisitions of other companies, is vital to the debate over its future. Short sellers and other critics, for example, have argued that the company’s drug brands are, in the main, declining; without the torrid pace of acquisitions, shrinking revenues and profits are a foregone conclusion.
Thus the importance of looking at what Philidor’s newly exposed captive pharmaceutical network reveals. Here’s what it shows: In the second quarter, Valeant’s 8-K reported “organic” sales growth of 19 percent, with revenue growing $691 million, to $2.73 billion from $2.04 billion.
Of this $691 million, however, at least $392 million was attributable to acquisitions, with the $299 million balance organic revenue.
The Kaufman declaration’s release of the Philidor/Valeant invoices to R&O imply a prospective quarterly sales run rate of about $55 million (an average $4.6 million weekly shipment multiplied by 12 weeks). This would have accounted for 18.5 percent of Valeant’s total organic growth in the second quarter. From there, it’s a sure bet that given the prominence of West Wilshire to Philidor’s billing unit, its sales volume would easily surpass R&O.
Notionally, organic growth equal to 40 percent or more of that $299 million could have come from two pharmacies that even the most gimlet-eyed Valeant sleuth didn’t suspect existed.
It also becomes much easier to understand why Valeant’s management didn’t immediately sever the relationship with Philidor.
————————
An outside spokeswoman for Valeant, Renee Soto of Sard Verbinen, told the Southern Investigative Reporting Foundation last week the company would not comment.
A message left for Gary Tanner was not returned.
And attempts to contact Eric Rice and other Philidor employees named in the story by placing calls to the company’s management ended up with their being routed to Greg Blaszczynski, the chief financial officer of BQ6 Media. That’s the pharmaceutical marketing effort where both Davenport brothers have served as CEO.
If the name Valeant Pharmaceuticals International doesn’t ring a bell, its business practices should. The Quebec-based drug manufacturer’s policy of implementing regular price increases that often run north of 100 percent has generated plenty of anger, a congressional investigation, constant press coverage and a subpoena from the U.S. attorneys’ offices in both the Southern District of New York and the District of Massachusetts.
But as strange as it may seem, a slim legal filing in California federal court is poised to make Valeant’s world rockier still.
The story starts 50 miles northwest of Los Angeles in Camarillo, California, with R&O Pharmacy, a modestly sized operation co-owned by veteran compounding pharmacists Russell Reitz and Robert Osbakken.
According to a lawsuit filed by R&O, Russell Reitz received a letter from Robert Chai-Onn, Valeant’s general counsel and director of business development, requesting repayment of $69.8 million for “invoiced amounts.” This apparently struck Reitz as odd since R&O had done no business, at least in any direct fashion, with Valeant. Moreover, he had never received a single invoice from Valeant or its subsidiaries.
Reitz forwarded the letter to Gary Jay Kaufman, his lawyer in Los Angeles, who sent a letter to Chai-Onn on Sept. 8, noting that the lack of invoices from Valeant indicated to him that one of two things was happening: Valeant and R&O were being jointly defrauded by someone, or Valeant was defrauding R&O. He suggested they talk it over by phone.
Chai-Onn never responded, and on Oct. 6 Kaufman filed suit, seeking a determination from the court that R&O owes Valeant nothing.
There is, however, a hook, and as these things go, it’s a big one: The Southern Investigative Reporting Foundation has confirmed that Reitz was indeed doing business of some sort through a company called Philidor Rx Services and a man named Andrew Davenport.
Which makes Valeant’s demand letter very interesting.
To understand why, it’s important to understand what Philidor is. To the public, it describes itself as a “pharmacy administrator” and, according to a call service operator last Thursday, Valeant is its only client. Located in Hatboro, Pennsylvania, about 30 miles outside Philadelphia, Philidor noted in its corporate filings that both companies are independent of each other.
The phrase “pharmacy administrator” appears to be, in Philidor’s case, a term of art.
A better description is a “specialty pharmacy,” that fills, ships and obtains insurance approval for prescriptions of the more complex drugs Valeant makes. During its third-quarter conference call last year, the only instance when Philidor has been publicly mentioned by an analyst, Valeant chief executive Mike Pearson said that perhaps 40 percent of its business flows through specialty pharmacies. In July he reiterated the company’s guidance for up to $11.1 billion in 2015 revenue, suggesting that as much as $4.4 billion in product could move through this Philidor channel.
(Note that specialty pharmacies are exempt from reporting the drugs they sell to IMS Health, the tracking service used by companies and analysts to monitor drug sales and inventory channels.)
As is the case with many private companies, the financials of Philidor are hard to come by, but it is unmistakably an operation of some mass, with about 900 employees and its own legalunit. A Pennsylvania state senator posted an April 6 interview with company CEO Andy Davenport in which he stated the company was on track to process 12,000 to 15,000 prescriptions daily by December. With prescription costs regularly running into the hundreds and even thousands of dollars, the company could potentially handle upward of $1.5 billion in product this year.
Here’s a key cog in Valeant’s “patient access” program: Patients referred to Philidor often receive coupons for reduced or waived co-pay requirements (given to the prescriber by Valeant’s sales representatives). And, in turn, Philidor would appear to attempt to recoup the cost of the drug from private insurers or Medicare. Theoretically, this makes price increases less risky for Valeant, given that a sizable population of a drug’s users frequently don’t have the capability to observe them. Still, the patient access program is central to the company’s distribution program, and one of the issues the U.S. attorneys’ subpoenas specifically sought information about.
Philidor’s business practices have generated mixed reviews (at best) on consumer message boards — including numerous instances of alleged unwanted refills and an allegation of the improper removal of HSA funds. Another message board account alleges that to get reimbursement approvals, prescriptions already denied at larger insurers were “pushed through” their sister pharmacies. (To be sure, comments on these sites can be gamed, both by consumers and the company, and the Southern Investigative Reporting Foundation was unable to verify these accounts.)
Several questions remain unanswered: On the assumption that there is $69.8 million due someone, why wouldn’t Philidor’s two in-house attorneys have issued a demand letter to R&O? Similarly, why wouldn’t Valeant’s high-profile general counsel, when challenged, not provide support for his demand and avoid the risk and expense of litigation? Additionally, if Valeant does have some sort of claim to that nearly $70 million, what then is their real relationship to Philidor?
————————
The Southern Investigative Reporting Foundation was able to uncover Valeant’s financial connection to Philidor — one that it hasn’t disclosed to investors — as laid out below.
The first task was to establish who owns Philidor. What we discovered was indeed revealing, albeit probably not in the way its owners intended.
Put bluntly, Philidor has gone to great lengths to conceal its ownership. Start with a man named Matthew Davenport, the listed principal on most of Philidor’s state registrations; additionally, several states list David Wing, John Carne and Gregory Blaszczynski as officers, and a few more have an End Game Partnership LLP listed as an assistant treasurer.
Given Andy Davenport’s video above, his role as Philidor’s chief executive is clear. Plugging the address of End Game Partnership LLP (which in turn is owned by End Game LLC, a Las Vegas-based entity) from its filings into a search engine turns up a match to a house Andy Davenport owns in Horsham.
A Southern Investigative Reporting Foundation phone call to Philidor’s administration revealed that there is no Matthew Davenport, David Wing, (Edward) John Carne or Gregory Blaszczynski working at Philidor. On the other hand, all four work at BQ6 Media, a pharmaceutical marketing company located about 2.5 miles from the company. At one point, prior to Philidor, Andy Davenport was its CEO. Both BQ6 and Philidor share the same domain registrar, Perfect Privacy LLC. The company’s LinkedIn profile lists 28 employees but the majority are consultants or contract workers, with several listing time spent at Philidor.
The Philidor state registration in North Carolina was particularly helpful in that it listed a broader array of owners than other states.
David Cowen is a former hedge fund manager and Elizabeth Kardos is general counsel for restructuring consultants Zolfo Cooper who are married and own Four Beads LLC; they did not return a message left at their house or reply to an email sent to Kardos. Nick Spuhler is a BQ6 alum who could not be reached, David Ostrow is a physical therapist and golf swing coach who did not return multiple calls to his house and residence, Jeffrey Gottesman is an insurance agent who has a sideline as a competitive poker player; reached on his mobile phone, he declined comment. The address listed for Gina Miller tracked to a code inspection business with no apparent connection to Philidor. Alternatively, a Gina Milner works at BQ6, but it couldn’t be determined if she is involved. Fabien Forrester-Charles of Hatboro, Philadelphia, and Francis Jennings of Naples, Florida, could not be reached, and Michael Ostrow of Bala Cynwyd, Philadelphia, did not return a voice message left at his house. Paula Schuler of Old Greenwich, Connecticut, listed as an owner along with her husband Timothy, said she couldn’t talk at that moment; she never returned two follow-up calls.
It is not readily apparent if there are any specific relationships among group members, beyond the general ties to Matthew and Andy Davenport (according to an online database they appear to be brothers), BQ6 and Philadelphia. One that does jump out is David Cowen and Andy Davenport’s tenure together at hedge fund Quasar Financial between 2004 and 2008; Davenport also donated to the Museum of American Finance, where Cowen is the president.
Not every state looked kindly upon the way Philidor went about securing out-of-state pharmacy operation privileges. California took exception to Matthew Davenport’s attempt to register as Philidor’s principal and rejected the company’s application for a Non-Residency Pharmacy Permit in May 2014. The state’s Department of Consumer Affairs Board of Pharmacy cited a series of disclosure-related problems, specifically his swearing to what was termed “false statement of facts” on the application, several of which involved the failure to disclose Philidor’s ownership group, as well as Andrew’s 27 percent ownership stake.
(A brief aside: Francois-Andre Philidor was an 18th-century French chess master, who wrote a book about it, “The Analysis of Chess.” BQ6 Media is named after the chess shorthand for Bobby Fisher’s legendary move against Russian chess master Boris Spassky in 1972. Another popular chess move is the King’s Gambit Accepted, or as it’s often referred to in chess notation, KGA.)
Establishing the economic connection between Valeant and Philidor was less time-consuming.
As it happens, Valeant has a wholly owned unit named KGA Fulfillment Services Inc., that was formed in Delaware in November 2014. Its only mention in any Valeant filings is that sole line in last year’s annual report. An exhaustive search didn’t turn up any references to it in trade publications, nor state and federal databases. (What the initials stand for, apart from the similarity to the chess strategy, is unknown.)
The Southern Investigative Reporting Foundation found KGA Fulfillment Services listed as the “secured party” on UCC-1 liens placed this January and February against the members of Philidor’s ownership group. These liens are the public notice that a lending entity may have an interest in the debtor’s personal property. In this case, Valeant/KGA lent money to Philidor’s ownership group, and per the rules is announcing that their equity stakes in Philidor are potentially collateral.
That an important financial relationship exists between Philidor and Valeant’s KGA unit is inarguable; why it exists is much less clear. From the standpoint of rational self-interest, the owner of a rapidly growing business would almost never want to borrow against their equity stake, let alone from the newly launched subsidiary of the enterprise’s sole customer.
————————
Over several days, since coming across the California lawsuit, the Southern Investigative Reporting Foundation made repeated phone calls to every person or company discussed above. With the exception of Jeffrey Gottesman from the Philidor ownership group and R&O Pharmacy’s lawyer, Gary Jay Kaufman — who both declined to comment — every other person did not return our calls.
Robert Chai-Onn did not reply to a call to his office; a call to a mobile phone registered to his name was answered by his wife, who said she was on the West Coast and was unsure where her husband was at that moment.
Meghan Gavigan of Sard Verbinnen & Co., an outside spokeswoman for Valeant Pharmaceuticals, was unable to secure a response from the company.
Slowly but surely answers to the many riddles of how Insys Therapeutics could achieve its mercurial success are beginning to emerge.
The Scottsdale, Arizona-based pharmaceutical company has only one commercial offering, a sublingual Fentanyl formulation called Subsys, whose sales growth has managed to double its market’s size, to more than $500 million from an estimated $225 million since its approval and launch in March 2012, according to executives at rival companies. In turn, the upward march of the company’s share price has turned its growing legion of supportive brokerage analysts and money managers into minor geniuses. (Southern Investigative Reporting Foundation readers will recall Insys from an April 24 investigation of the drug’s mounting number of lethality cases and the company’s unusual marketing efforts.)
Therein lies the rub.
Subsys is approved only to treat breakthrough cancer pain. The market for such drugs was estimated to have an annual growth rate of about 10 percent in the spring of 2012, according to former Insys sales staff and rival pharmaceutical executives. Instead, on March 21, 2014, about two years after its launch, Subsys managed to nose past Cephalon’s Actiq, then a leader in this narrow category, in number of prescriptions written, according to IMS Health data obtained by SIRF; last September Subsys took the lead for good.
These opioid drugs are so potent that the Food and Drug Administration created a stringent prescription protocol for them (known as TIRF-REMS), with multiple steps for a patient to go through before a prescription is dispensed.
Yet according to Medicare Part D records for 2013, no oncologists appear on the list of Subsys’ biggest prescribers.
Given this apparent lack of support from oncologists, it appears odd that insurance companies seem to have embraced Subsys, continually approving its reimbursement at a level none of its competitors can obtain. A leading Subsys prescriber told the Southern Investigative Reporting Foundation that in his estimation, “Insurers cover over 90 percent of [Subsys prescriptions] for at least one [90-day] cycle,” whereas rival drugs appear to have an approval rate hovering at 33 percent. The doctor’s account of a chasm between how insurers treat Subsys and how they deal with its rivals was corroborated by a senior executive at an Insys rival and three former Insys sales staff members.
But it was not until records in the Centers for Medicare & Medicaid Services Open Payments database were released in October 2014 — covering the last five months of 2013 — that a linkage could be more readily detected between the volume of Subsys prescriptions and payments to doctors.
As Insys’ share price continued to trend upward, Wall Street’s brokerages found it easy to promote the company’s business practices, as a Jefferies research report from December shows.
But now federal prosecutors are peeling back the veil to reveal a black world behind Insys’ earnings. The initial results suggest they do not condone what they are seeing.
————————
Dr. Gordon Freedman, a 55-year-old anesthesiologist, is in every way imaginable a member of New York’s medical establishment, with a busy two-office practice and, until very recently, a faculty appointment at the Mount Sinai School of Medicine.
A graduate of the Sackler School of Medicine, Dr. Freedman resides in Irvington, N.Y., a pretty village along the Hudson River just 20 miles north of Manhattan. This seems to be the perfect capstone to a life that outwardly evinces the virtues of taking initiative and pursuing hard work.
But in life, as in medicine, the mechanics of how the system works matter. And for Dr. Freedman, the road to success has been paved with lots of Insys’ cash.
The June 30 update to the Centers for Medicare & Medicaid Services Open Payments database included the full amounts of pharmaceutical company payments in 2013 and 2014 to doctors for entertainment and speaking at corporate events and for research. The database revealed that in the last two years Insys spent almost $204,000 on Dr. Freedman, with more than $147,000 of that being for speaking programs last year in 52 separate payments of $2,400 to $3,750, not including food and travel expenses; none of the money was for research.
Was paying Dr. Freedman so much a good investment for Insys? Probably — at least initially.
Medicare Part D records show that in 2013, the most recent year for which data is available, Dr. Freedman ranked as the 15th-highest Subsys prescriber as measured by dollar amount, having written 35 prescriptions that cost Medicare $393,961. The Southern Investigative Reporting Foundation, via a database tracking TIRF-REMS prescriptions, identified 60 Subsys prescriptions that Freedman wrote from March 2012 (when Insys obtained FDA approval to sell the drug) to the end of December 2013.
The math behind a typical prescription shows why Insys has not been hesitant to pay prescribers to talk about the drug. In 2013 the wholesale acquisition cost of a 90-day supply of Subsys of 400 micrograms, statistically the most frequently prescribed amount according to Wolters Kluwers data, cost $4,608. In 2014 at a blended cost of $58.68 per unit (there was a midyear price hike), that same 90-day supply cost $5,281. Currently, priced at $97.80 per unit, a prescription costs $8,802. (These figures do not take into account frequent discounts.)
The Southern Investigative Reporting Foundation repeatedly reached out to Dr. Freedman to discuss his speaking engagements but he did not return multiple calls to his home, office or cell phone; he also did not reply to an email sent to his Mount Sinai address.
In response to questions about the ethics of Dr. Freedman’s Insys payments, Mount Sinai spokeswoman Elizabeth Dowling emailed the following statement: “Dr. Freedman is not employed by Mount Sinai and we do not have access to the details of his personal relationships with non-Mount Sinai entities.” She did not reply to follow-up questions.
As the chart below indicates, Dr. Freedman was hardly alone in profiting from Insys’ gravy train; 12 other doctors received more than $100,000 last year from the company.
Medicare rank is determined by the value of Subsys prescriptions written by the doctors.
The nearly $7,390,872 that Insys spent last year on payments for what it calls “compensation for services other than consulting” — with $6.3 million going to doctors and the almost $1.1 million balance for travel and entertainment costs — stands out from the practices of its competitors marketing TIRF-REMS drugs. The $7 million sum represents 7.2 percent of Insys’ 2014 selling, general and administrative expenses, with the speaker payments amounting to 2.9 percent of its total sales.
In comparison, Galena BioPharma, the maker of Subsys competitor Abstral, spent just $132,372 on what it calls “honoraria,” representing 0.4 percent of selling, general and administrativeexpenses, with speaker payments amounting to 0.8 percent of total sales. (To be fair, Depomed, the maker of Lazanda, spent $206,250, or 3 percent, of its almost $7 million in sales on speakers.)
When the Southern Investigative Reporting Foundation interviewed Insys’ sales chief Alec Burlakoff in April, he bristled at the suggestion of a quid pro quo between prescription-writing volume and speakers program compensation. As he saw it, the speakers program was the pharmaceutical industry version of a university’s faculty lounge, where colleagues could discuss the latest approaches and innovations in their discipline (albeit one where the conversations are shaped by frequent payments of thousands of dollars, as opposed to a reinterpretation of Sylvia Plath).
“Putting board-certified doctors together, where one of them is explaining the benefits he or she is seeing” [from prescribing Subsys] was the key to the company’s remarkable sales growth, Burlakoff said.
But federal prosecutors have recently served notice that they are taking a very different view of Insys’ speakers program. In a pair of cases in Connecticut and Alabama, assistant U.S. attorneys have removed some of the basis for support of the company among brokerage and investors by definitively linking three of the most highest-volume Subsys prescribers to Insys’ payments of “bribes” and “kickbacks” in open court.
————————
In Hartford’s U.S. District Court on June 23, nurse practitioner Heather Alfonso of Derby, Connecticut, pleaded guilty to accepting $83,000 in bribes from a pharmaceutical company that were designed to influence the choice and amount of prescriptions she wrote. According to an account of the proceeding, the company was identified as Insys and the payments were made under its speakers program.
Apart from the connection of the speakers program to bribery, Alfonso’s surrender of her prescription-writing licenses means Insys loses another important prescription writer, in the latest round of the cat-and-mouse type contest between law enforcement and the high-volume writers of Class II opioids prescriptions. She was the 22nd-highest Subsys prescriber in 2013, according to Medicare Part D data, and ranked 25th in Tricare records in 2014.
Alfonso, in her plea, admitted to having been paid for her attendance at 70 separate speaker dinners, with the prosecutor describing them as either having no doctors or physician assistants in attendance — and thus no educational value — or as meals with only her Insys sales representative and friends in attendance.
The plea completes a remarkably tumultuous six-year span for Alfonso. In July 2009, with five children and her parents claimed as dependents, she sued for protection from creditors under Chapter 7 of the bankruptcy code, listing $424,682 in assets and $525,316 in liabilities.
According to Alfonso’s plea agreement, she is potentially facing 46 to 57 months in prison but the prosecutors reserve the right to request that a judge adjust that figure, presumably downward. None too subtly, this means that Alfonso has a remarkable incentive to negatively portray Insys and its sales practices.
Reading between the lines of the press release announcing Alfonso’s plea, however, an observer could infer that federal prosecutors are expanding the investigation beyond the bribery plea into insurance fraud.
“Interviews with several of Alfonso’s patients, who are Medicare Part D beneficiaries and who were prescribed the drug, revealed that most of them did not have cancer, but were taking the drug to treat their chronic pain,” according to the release. “Medicare and most private insurers will not pay for the drug unless the patient has an active cancer diagnosis and an explanation that the drug is needed to manage the patient’s cancer pain.”
To whit: Alfonso’s patients received Subsys despite the absence of a cancer diagnosis; without it, a refusal of coverage is nearly automatic within the field. Thus the granting of insurance reimbursement could imply that somehow the diagnosis codes of these patients were changed.
This also speaks to what the unnamed physician referenced above, about Subsys prescriptions’ being approved by major commercial insurance carriers and Medicare much more frequently than prescriptions of rival medications were.
On investor conference calls, Insys CEO Michael Babich has mentioned a dedicated prior authorization unit that works closely with a prescriber’s office and sales staff to assist with paperwork. But other rivals do this, too, and while Insys might realize more efficiencies, it seems unlikely that the company is almost three times better at this.
One possible answer is provided in a class action (recently settled for an undisclosed amount): A confidential witness from Insys’ prior authorization unit claimed that staff people were trained to impersonate prescriber office staff when talking to pharmacy benefit-management companies, lie about the previous drugs taken by the patient (most insurers require patients try a generic drug and have it fail before a branded drug is approved) and tailor diagnoses to insurers, based on internal records of prior approval rates.
Insys never responded to these charges prior to the class action’s settlement.
Another possible explanation lies with the remarkably close working relationship that Insys has with a drug distributor called Linden Care, based in Syosset, New York. Former sales executives describe this bond as much closer than the standard vendor-distributor relationship, such that any issue with a prescription could be rapidly cleared up and, despite the multiple checks and balances within TIRF-REMS, the drug appear at the patient’s door within 24 to 48 hours. Linden Care has recently been put up for sale by its owner, BelHealth Investment Partners. A phone call to Inder Tellur at BelHealth was not returned.
————————
Alfonso’s legal predicament pales in scope next to the May charges filed against two pain-management physicians, Dr. John Couch and Dr. Xiuliu Ruan, partners in Physician’s Pain Specialists of Alabama in Mobile. Ranking as No. 3 and No. 6, respectively, as prolific Subsys prescribers through Medicare, in 2013, and second and first as Tricare prescribers for 2014, the pair had almost certainly become the company’s largest single revenue source.
With the two doctors arrested and charged with conspiracy to commit health care fraud and for distributing controlled substances, prosecutors released a few weeks ago a pair of affidavits that the Federal Bureau of Investigation special agents who led the investigation had filed.
Both agents described a veritable Class II drug prescription-writing factory, with prescriptions being written every four minutes and almost no medical analysis occurring from the harried physician assistants who saw the majority of the clinic’s patients. Undercover agents posing as patients with demonstrably false injury claims were barely examined yet received multimonth subscriptions for Class II drugs.
FBI Special Agent Amy White said that a confidential informant employed by Dr. Couch and Dr. Ruan described their participation in a pharmaceutical company’s speakers program as being “paid for promotion.” (While Insys was not named specifically, thc company’s identity can be deduced given the amount and timing of the payments cited.)
Similar to Alfonso’s case, the Insys speakers program is portrayed in the FBI agents’ affidavits as little more than Dr. Couch’s and Dr. Ruan’s being paid thousands of dollars for having dinner with their sales representative, according to the confidential informant. (A former Insys sales representative told the Southern Investigative Reporting Foundation that Dr. Couch and Dr. Ruan have been personally close for a decade to their Insys representative, Joe Rowan, whom they also dealt with at Teva Pharmaceuticals.)
Agent White’s affidavit alludes to the possibility that Dr. Couch abused the same class of drugs he so frequently prescribed. In a joint operation with a county drug task force, the FBI obtained the content of the trash from Dr. Couch’s residence and found that several syringe and Subsys packages had been discarded. Additionally, a confidential witness told the FBI of observing used syringes in the restroom of Dr. Couch’s personal office. Dr. Couch has a history of alcohol and prescription drug abuse, per his testimony in a California Medical Board account of the probationary certificate he was awarded in 1995, while completing a one-year pain-management residency at UCLA.
Another FBI special agent, Michael Burt, said he estimated that 50 percent to 60 percent of the clinic’s gross proceeds were derived from fraudulent activities. He said payments from Insys were found in several personal bank accounts of Dr. Couch and Dr. Ruan that he sought to seize. Another account of Dr. Ruan, Burt said, contained “kickbacks” from Industrial Pharmacy Management, a drug distributor whose founder Michael Drobot pled guilty in February 2014 to a $500 million insurance fraud scheme.
The Southern Investigative Reporting Foundation sought comment from Dr. Couch and Dr. Ruan. Neither doctor replied to multiple attempts to obtain comment.
Dennis Knizely, Dr. Ruan’s defense counsel, did respond, however, saying his client has been unfairly targeted: “These are baseless accusations, centered on the government’s interpretation [of complex issues] only. We will fight this at trial and show the government to be wrong.”
Added Knizely: “Dr. Ruan’s patients had many medical problems, including cancer, serious auto and work-related injuries. I have no doubt insurance companies have a problem with him; he ordered specific and complex procedures done to ensure the best care for his patients. His medical decisions will be shown to be sound and compassionate.”
John Beck, Dr. Couch’s lawyer, did not return multiple calls seeking comment.
————————
One of the odder elements in Insys’ operations has been its relationship with key sales executives. In April the company sued two salespeople, Lance Clark and former Western region sales chief Sunrise Lee, for purportedly maintaining outside jobs. The company has since amended its claim against Clark but dropped the suit against Lee. A call to Clark was not returned; an inquiry to Lee was referred to her lawyer, Stephanie Fleischman Cherny, who did not respond to a request for comment.
In addition, on May 8 Insys sued Michael Ferraro, a sales representative covering southwest Connecticut for maintaining an outside interest in a compounding pharmacy. On May 28 Ferraro filed a response, claiming that he had fully disclosed his interest in the pharmacy, that he was winding it up and that he had notified the company of a series of what he alleged were federal violations stemming from an April 17 lunch with his district supervisor, Michelle Breitenbach. On July 10 Insys dropped its suit against Ferraro.
Prior to the July 4 holiday weekend, Insys dismissed Fernando L. Serrano, Dr. Freedman’s sales representative. Serrano’s LinkedIn profile mentions a stint at JPMorgan Chase as a mortgage banker but not a 2012 stint at two heavily sanctioned boiler rooms, Aegis Capital and John Thomas Financial (a firm expelled from the securities industry by the Financial Industry Regulatory Authority in 2015, along with its founder). Serrano told the Southern Investigative Reporting Foundation that he was still in shock about his Insys dismissal.
A former Insys sales executive said that the large amounts of Subsys prescriptions written by Dr. Freedman and other prescribers that Serrano had called on in 2014 had propelled him into the top-tier of revenue generators.
Serrano declined to elaborate upon why he left Insys, other than saying, “It’s just insane” several times. A follow-up call was referred to his lawyer, Ali Benchakroun, who declined to comment.
An email to Insys sales chief Alec Burlakoff and New York regional sales manager Jeff Pearlman seeking comment about the reasons for Serrano’s dismissmal were not returned.
The Southern Investigative Reporting Foundation left a voice message for Insys CEO Michael Babich and sent an email with a series of questions. He did not reply.
Additionally voice messages and emails (when addresses could be found) were sent to the top 10 doctor recipients of Insys payments in 2014 but none responded.
On the evening of July 1, 2014, Carolyn “Suzy” Markland, a 58-year-old Jacksonville, Florida, resident with a degenerative disc disease, took her prescribed medicine — a 400-microgram dose of a Fentanyl spray called Subsys — and went straight to bed.
Despite the fact that she regularly experienced pain, taking Subsys was not an everyday affair for Markland. Her prescription had been filled several months prior but she almost never took the stuff; her longtime family doctor and pharmacist had expressed to her plenty of no-holds-barred skepticism about it. On the three occasions she had taken Subsys, her family noticed that its sedative and respiratory effects were noticeably sharper than those of another strong painkiller she took, Exalgo.
On July 2, Markland visited Dr. Orlando Florete, her pain-management physician of five years, for a scheduled injection for her lower spine. As part of her anesthesia mix prior to the procedure, she received another Fentanyl dose. Unlike what was the case after previous procedures, however, she wasn’t up and moving some 20 to 30 minutes afterward; this time it took about an hour until her oxygen levels allowed for her to be safely released.
Markland was tired for the balance of the day and headed to bed early, skipping her usual cup of decaf beforehand.
She never woke up.
With Markland pronounced dead at 7:01 a.m. on July 3, the Jacksonville medical examiner’s office listed the cause of her death on its report as “drug toxicity,” noting the presence of Fentanyl and Exalgo. Her death was classified as “accidental.” The report also noted that Markland’s family doctor refused to sign the death certificate; Dr. Florete did.
Bob Markland, Carolyn’s husband of 19 years, declined to comment apart from providing a timeline of her Subsys use.
The medical examiner’s report of a lethal combination of Fentanyl and other drugs in Carolyn Markland’s blood is puzzling and sad, seemingly emblematic of a strain in modern American medicine whereby solutions to pain can be as scarce as the medication for that pain is abundant.
In another sense, this tale recounting Dr. Orlando Florete’s treatment presents a parallel trend in American medicine — that of the physician as a compensated endorser. According to figures from the Center for Medicare & Medicaid Services’ Open Payments database for the last five months of 2013, Florete was paid $18,874.03 by Subsys’ manufacturer to travel and speak to fellow doctors. The firm is a small but rapidly growing pharmaceutical company called Insys Therapeutics.
Additionally, the 16 Subsys prescriptions written by Dr. Florete from Jan. 1, 2013, to May 31, 2103, according to documents obtained by the Southern Investigative Reporting Foundation through the Freedom of Information Act, cost the U.S. military primary health insurance plan Tricare $133,770.36.
Pharmaceutical companies’ compensating physicians for discussing their product — or even attending carefully scripted seminars — is a longstanding, and legal, practice. To be certain, many within the medical community have been concerned about this for a while, and in 2013 regulations were put in place to ensure disclosure of all physician payments. (Pro Publica has published a wealth of information on the issue.)
A phone message seeking comment from Dr. Florete about his relationship with Insys and his Subsys prescription writing was not returned by the time of publication.
Like Dr. Florete’s speaking engagements, another unremarked-upon issue was the nature of Carolyn Markland’s Subsys prescription. The drug indicated to treat breakthrough cancer pain was prescribed for a bad back. The law affords doctors great latitude in determining whether drugs can be prescribed for reasons other than what they are designed for. On the other hand, doctors’ writing prescriptions based on off-label marketing have been at the center of nearly two dozen False Claims Act cases in the past 20 years, resulting in more than $13 billion in pharmaceutical company fines and settlement payments.
In the case of Subsys, its official label — indicated by the folded paper insert with the impossibly small typeface that comes with the package — notes that it’s contraindicated for those with headache pain and people not tolerant of the opioid class of drugs. According to the Centers for Disease Control and Prevention, 175,000 people died from some form of prescription opioid abuse from 1999 to 2010 compared with 120,000 from heroin and cocaine overdoses.
Like Dr. Florete, Insys Therapeutics has been doing pretty darn well. The company has had a remarkable level of financial success and its soaring stock price, as shown in the chart below, has made it a darling on Wall Street.
But that level of growth ought to warrant a raised eyebrow: Achieving in just two years more than $222 million in sales (from a level of about $15.5 million) without having invented something like a better search engine is no mean feat. Fentanyl, after all, has been around for many years. And while Subsys is the only spray version available, several Insys competitors are well-established and better capitalized and have sales forces that reach all 50 U.S. states.
While details about this breakthrough cancer pain medication are hard to find, or at least ones that are not self-serving management hype, veteran sales staff members from Insys and other pharmaceutical firms projected the company’s future growth rate to be roughly 10 percent a year. If this ends up being the case and the company is selling to oncologists, then the growth possibilities for Insys should be a function of that plus whatever business it can take away from its larger competitors. Many companies would be happy for those odds.
But Insys’ revenue grew north of 100 percent: Whatever organic growth the company is achieving is being aided by a whole lot of doctors who have grown profoundly fond of an expensive drug that’s accompanied by an acre of governmental red tape and one that the largest pharmacy benefit managers will no longer touch.
The question then becomes “how?”and “why?”
An investigation of Insys by the Southern Investigative Reporting Foundation reveals that this growth has come at a remarkable price: Food and Drug Administration data shows that Subsys is proving lethal to a growing number of patients, many of whom, like Carolyn Markland, are taking it for so-called off-label indications, such as headaches and back pain.
In reporting this story, the Southern Investigative Reporting Foundation repeatedly encountered former Insys employees who had received subpoenas requiring their appearance in front of a Department of Justice grand jury that has been empaneled in Boston. Still others had been interviewed for an investigation of the Department of Health and Human Services’ Office of the Inspector General.
A company that has been killing it — at least financially — is clearly in a lot of trouble.
————————
To understand Subsys, the first thing to know is that it is literally a drug apart: a Schedule II spray administered below the tongue and dozens of times stronger than morphine; its effects are profound, especially within the respiratory system, and almost immediately. Which is the point, of course, given that many people with cancer experience nausea and cannot take pills.
To address the twin risks of addiction and overdose, in March 2012 the Food and Drug Administration began what it calls the Transmucosal Immediate Release Fentanyl Risk Evaluation and Mitigation Strategy, blessedly shortened to TIRF-REMS. At its heart, the program is designed to make obtaining a prescription for Subsys (and five other drugs) a very deliberate process, with built-in checks and balances, such as confirmed opioid tolerance, signed patient statements and use of specially certified doctors and pharmacists.
No one, in other words, is dropping off a Subsys prescription at, say, a CVS pharmacy’s drive-through window.
Despite the unusual amount of federal guidelines designed to safeguard patients, Subsys is no stranger to adverse events.
The Southern Investigative Reporting Foundation asked Adverse Events, a California-based consultancy that collects and analyzes drug side effect data to analyze the FDA’s Adverse Event Reporting System’s tracking of fatalities related to Subsys. (In medical terms, an adverse event is defined as an undesirable outcome related to a drug’s use and includes categories in addition to death.)
The analysis shows Subsys was referenced in 63 adverse event reports resulting in deaths since its January 2012 FDA approval. Participation in the FAERS database is voluntary — a prescribing physician might not learn of an adverse event related to a drug; others elect not to report them. Because of this, many in the medical industry argue — privately — that FAERS’ data skews toward the lowest potential occurrence rate.
Given the relatively sparse amount of FAERS data that the Southern Investigative Reporting Foundation obtained (just age, gender and date of death are provided), placing the death of 63 Subsys users in a broader context is not so cut-and-dried. Certainly it’s reasonable to suppose that a percentage of those prescribed Subsys have cancer and would naturally have a higher rate of mortality. Some FAERS entries list Subsys along with one or two additional drugs. But dying of cancer isn’t usually considered an adverse pharmacological event; dying of respiratory failure when taking Subsys for a migraine is.
So how has Insys managed to grow exponentially?
The answer appears to have multiple parts: a truly unique sales force paired with a corporate speakers program that provides a stream of ready cash to frequent prescription writers.
————————
There’s no way around it: Insys’ sales force is very different from its competitors in the pharmaceutical industry. One reason is that a pharmaceutical sales background or even college courses in science are not required. Another is that if a candidate appears to be driven and aggressive, the company will look past things that a local Starbucks might not.
Scrolling through the LinkedIn profiles of Insys sales reps lends some credence to one of the assertions in an amended class action filed against the company in October that was settled the past week without a disclosure of the terms. The class action asserted that that Insys’ sales force was selected not for background or skill but for physical appeal
According to a summation of three confidential witnesses in the class action by the plantiffs’ lawyer, “most of Insys’s sales representatives were extremely attractive women.” (To be fair, Merck and other leading pharmaceutical companies have long drawn attention for constructing sales forces with a large percentage of attractive women.)
Then there’s the sales head of the New York region, Jeff Pearlman. Before becoming what his peers say is a highly productive salesman of Schedule II opioids, he was the marketing and sales chief of a company that sold aquariums.
Prior to that, he ran a ticket sales agency called Sitting Pretty Seating Services, which, in 2004, attracted the attention of the New Jersey Division of Consumer Affairs. Shortly afterward, the company’s registration was revoked after it did not file an annual report for two consecutive years, records indicate.
After this article’s initial posting, Pearlman said he had medical sales experience, having worked in the late 1990s for a company that sold diagnostic testing equipment to detect sleep apnea as well as for a company that sold genetic endocrinology testing devices in the mid-2000s.
Sunrise Lee, the recently departed head of Insy’s central and later Western sales region, offers an example of the company’s willingness to take a shot on a profoundly nontraditional prospect.
Prior to her stint with Insys, she was a dancer at Rachel’s, a West Palm Beach strip club. (She is the person at the far left top photo, taken from Rachel’s Web site, in this set; the bottom photo, from Facebook, shows a Insys sales outing at Chicago’s Wrigley Field for its top revenue producers.) It’s not clear what Lee did before adult entertainment.
About a year after Lee started selling one of the six drugs so lethal that the FDA had created a separate prescription protocol to monitor them, Insys promoted her to run the company’s Midwest sales.
SIRF asked Alec Burlakoff, Insys’ national sales chief, about the choice of Sunrise Lee to run sales for a quarter of the American land mass.
While agreeing with SIRF’s assertion that the adult entertainment world is not a traditional recruiting ground for pharmaceutical companies, Burlakoff offered that Lee had unusual attributes that were helpful in marketing Subsys to doctors.
“Doctors really enjoyed spending time with her and found Sunrise to be a great listener,” Burlakoff said.
“She’s more of a ‘closer,’” he said, using the common sales term often invoked to describe someone who helps convince a wavering customer to purchase a product. “Often the initial contact [with a doctor] was made by another sales person.”
SIRF asked Burlakoff about the scenario of a former exotic dancer pitching a restricted drug to board-certified oncologists. He said she was more effective with pain-management physicians who appreciated what he referred to as her “empathy.”
“When you are dealing with [doctors] who are around pain and cancer all day, an empathetic and caring sales person is helpful,” Burlakoff said. He said that Lee had been involved in an unnamed nutriceutical company prior to joining Insys and speculated that her “holisitic approach” to the medical field might also have appealed to some physicians. SIRF, having no idea what that means, asked him to elaborate; he did not. (SIRF couldn’t find or identify the company.)
For her part, Lee declined comment about Insys, noting that she had just been sued by the company — as was also the case for Lance Clark, an Insys sales executive from Dallas who had reported to her — for violating corporate policy regarding outside employment. The suit alleged that she recruited physicians to use a toxicology testing company, Advance Toxicology, that was formed by Clark when he was still employed by Insys. It also alleged that she made up having earned a degree from Michigan State.
She did however confirm to the Southern Investigative Reporting Foundation that she has been in contact with both the Department of Health and Human Services’ Office of the Inspector General and “those other prosecutors,” perhaps referring to the Department of Justice in Boston. (She declined to discuss it further when asked for clarification.)
Clark, who was unaware of the suit until the Southern Investigative Reporting Foundation told him about it, declined to comment.
————————
When asked about Insys’ controversial business practices, especially alleged off-label sales and payments made to physicians under its speakers bureau program (covered in New York Times investigations), Burlakoff insisted that these portrayals don’t match how he and his colleagues conduct themselves on a daily basis.
“There is a very, very easy way to get fired on your first day at this company,” said Burlakoff, “and that is to mention selling off-label. We are only selling a breakthrough cancer pain drug. That’s all we want to address with a doctor.”
“You don’t run a unit at a company like this by cutting corners,” he said. (Burlakoff was fired from Eli Lilly in 2003 for his role in sending unsolicited samples of Prozac through the mail in a bid to boost the drug’s then slumping sales. He and several colleagues sued the company, alleging management had approved of the plan.)
Having worked for rival drugmaker Cephalon, Burlakoff said he has run [Fentanyl] training programs “for years” and makes it clear to members of the sales staff that their job is not to try to convince doctors but educate them about the benefits and possibilities of a drug that can help their patients cope with a cancer-fighting regimen.
(The Department of Justice fined Cephalon $425 million in September 2008 for its off-label sales practices, particularly of its Fentanyl product, Actiq; Burlakoff is referenced in a qui tamcomplaint filed in 2014, for allegedly ordering his staff to organize speakers program events to promote off-label prescription of its Fentanyl drug. He did not respond to a request for comment about this via email and voice messages.)
The Southern Investigative Reporting Foundation asked Burlakoff about his previous assertion that the primary market for the drug was oncologists.
“Yes, well, we are trying to break in to that market but most [oncologists] only care about the tumor or malignancy and, in my opinion, don’t focus on the pain component,” he said. “That’s a problem — for them and for us.”
Adding that among oncologists there is a “sense that prescribing [Subsys] is something for hospice,” Burlakoff said most oncologists that he and his colleagues deal with are happy “to refer pain treatment out” to pain-management doctors so they could focus on the cancer treatment.
SIRF asked Burlakoff if the pain-management physicians who appear to be prescribing upward of 90 percent of the drug are thus working in tandem with oncologists or are otherwise treating cancer pain. He replied that this was his understanding based on what members of his sales staff were telling him.
“I can say that no one at Insys wants to see anyone taking [Subsys] for anything other than cancer pain,” said Burlakoff. He went on to relate several feel-good stories about people whose lives have been changed because of Subsys. More substantively, he referred to discussions he has had with Insys founder John Kapoor, whose wife Edith died of cancer in 2005, that motivate him to sell a product that eases the suffering of cancer patients.
————————
Also misunderstood, according to Burlakoff, was the role of Insys’ speakers program in the company’s sales model. It wasn’t, as the class action alleged via a confidential witness, “a kickback program.” Nor was it the way to incentivize a series of pain-management physicians to write more prescriptions, as a New York Times article suggested.
Rather, “putting board-certified doctors together, where one of them is explaining the benefits he or she is seeing” from prescribing Subsys is the way that the drug gets acceptance. No sales rep is as effective as a doctor at convincing other doctors, he said.
“These are rich, highly educated doctors,” Burlakoff said. “They have money. Whatever they are paid isn’t material.”
SIRF asked Burlakoff if money was not the primary motivation for the doctors whom Subsys paid $25,000, $50,000 or more over the last five months of 2013, then what did he suppose it was?
The chart below of the top nine recipients of Insys payments, drawn from the Center for Medicare & Medicaid Services’ Open Payments data, paints a clear picture of doctors who have generated substantial income from the program. (See a list of the top 25 recipients of Insys payments.) Burlakoff did not reply to a request for comment on this data.
Many of Burlakoff’s former colleagues, however, described a very different experience with the speakers program.
A qui tam claim filed last year by former Insys salesman Ray Furchak alleged that the speakers program’s sole purpose was, in the words of his then supervisor Alec Burlakoff, “to get money in the doctor’s pocket.” The catch, Furchak alleged, was that the doctors who increased the level of Subsys prescriptions, and at higher dosages (such 400 or 800 micrograms instead of 200 micrograms), would receive the invitations to the program — and the checks.
The claim described texts from Burlakoff to Furchak and other sales colleagues regularly demanding that “doctors be held accountable” and that “doctors who are not increasing their clinical experience [prescription writing], please cancel, suspend, and cease doing speaker programs.”
The Department of Justice chose not to join Furchak’s suit and he withdrew it. Reached at his new job, Furchak said he stood by everything he had alleged but declined to comment further.
Conversations with former sales staff members support Furchak’s allegations that the speakers program was regularly used as a lever to pressure doctors to increase dosage strength as well as the frequency of their prescriptions for Subsys. In return, former sales staff members (who were granted anonymity in this story because of their involvement with the Department of Justice’s grand jury proceedings) often had to deal with doctors’ annoyance about payment levels or delays in receiving their checks.
The speakers program events have often been held at branches of Roka Akor, a tony sushi-steak restaurant company with venues in Scottsdale, Chicago and San Francisco that’s owned by Insys founder John Kapoor. Based on interviews with multiple attendees, the expenses often run into the thousands of dollars and, given the sheer number of events, have helped his restaurants capture a handsome revenue stream. An email to Insys CEO Michael Babich seeking comment was not returned by the time of publication of this article.
Former sales staff members also disagreed that Burlakoff’s full-throated rejection of off-label sales was shared by upper management. As evidence of this, two former salespeople pointed to a quarterly meeting in Atlanta for the Southeast region sales team in a June 2014 when CEO Michael Babich, during a question and answer session, read a question about the risk of off-label sales, given Cephalon’s steep penalty in 2008.
“I understand why you’re asking that question,” said Babich. “But Cephalon didn’t have TIRF-REMS; we do. You are protected because both the MD and the patient have signed it.”
Asked to elaborate, Babich said because of the TIRF-REMS requirement that the patient be extensively briefed on the risks of Subsys, there couldn’t be a plausible claim that the patient (or doctor) did not know what he or she were doing.
As one of the two attendees who described this event to SIRF put it, “There wasn’t much else to say about the issue when your CEO sees an information protocol as an insurance policy.”
Putting Insys’ assertions about serving cancer patients aside, the company’s bread is buttered by pain-management and physical-rehabilitation doctors, according to Tricare’s reimbursement and prescription data from Jan. 1, 2013, to May 31, 2014. Tricare represents about 9.5 million people, or 3 percent of the U.S. population.
Listed below are Tricare’s top 15 prescribers of Subsys.
Among the top 25 Subsys prescribers within the Tricare system, there are 20 pain-management physicians, one osteopath, one nurse practioner and three physician assistants. (See a full list of the top 25.)
The Southern Investigative Reporting Foundation attempted to contact Dr. Xiulu Ruan and Dr. Patrick Couch, partners in a Mobile, Alabama, practice, about the fact that they were the leading Subsys prescription writers by an impressive margin, to discuss this, as well as their ownership of C&R Pharmacy, which dispenses the drug to their patients. (About 50 percent of the Subsys dispensed in the United States is handled by Linden Care, a specialty pharmacy on New York’s Long Island, owned by Bell Health Ventures, a private-equity fund.)
Anthony Hoffman, a lawyer representing the practice, told the Southern Investigative Reporting Foundation, “Based on your representation of the [Tricare] data you discussed with my client, we believe it to be inaccurate and encourage you not to publish it.” He did not specify what was wrong with the data and declined to provide further comment.
————————
As first reported in The New York Times, a series of Insys’ leading prescribers have been at the center of serious allegations involving their prescription-writing practices.
Last May federal prosecutors filed a complaint against Gavin Awerbuch, a Michigan-based pain-management physician and the company’s largest prescriber under Medicare (and third most compensated), for allegedly bilking Medicare out of $5 million over several years. Prosecutors allege that he wrote 20 percent of the Subsys prescriptions dispensed to Medicaid recipients nationwide from 2009 to 2014. (Subsys, however, has only been FDA-approved since January 2012.)
In December 2013 Judson Somerville, a Laredo, Texas-based pain-management physician (the No. 8 prescriber under Medicare and the most compensated) had his prescription-writing privileges “temporarily suspended” by the Texas Board of Medical Examiners for a host of findings, including having three patients die with six months of 2012; it was not the first time he had regulatory trouble.
Stewart Grote, a Lansing, Kansas, pain physician and the company’s fourth biggest Tricare prescriber (he received $8,48.05 from Insys), was sanctioned for multiple standard of care lapses and is no longer registered as a physician in that state, according to licensing records; he also had an earlier regulatory issue in 2010.
The Florida Department of Health sued Paul Wand and Miguel de la Garza, the No. 11 and 23 Tricare prescribers, in 2012. (Wand received $20,169.06 from Insys; de la Garza $17,019.04.) The department alleged Wand’s standard of care did not meet professional standards for a series of patients, particularly with regard to his prescription writing. With respect to de la Garza, the department claimed he did not professionally administer care to one specific patient. According to the Florida Board of Medicine’s Web site, both cases appear to be ongoing.
Chicago-based pain-management physician Paul Madison is not among the top 25 Tricare prescribers but he was the 17th most compensated under the speakers program. He was indicted in 2012 in connection with an alleged $3.5 million false insurance billings scam. The case is ongoing.
Heather Alfonso, the 25th largest Tricare prescriber of Subsys and a Derby, Conn.-based nurse practitioner, surrendered her state and federal nursing and prescription-writing licenses within the past month amid a Connecticut Department of Public Health investigation into her conduct. A February Connecticut Health I-Team story reported that in 2012, the most recent year for which data was available, she was among the nation’s top 10 prescribers of Schedule II substances within Medicare’s drug program.
The Southern Investigative Reporting Foundation asked CEO Michael Babich for comment via a detailed voice message left on his office phone and a pair of emails. He did not reply by publication time.
Clarification:This piece has been updated to clarify the description of former work roles of Jeff Pearlman, Insys’ New York regional sales manager. He served as the sales and marketing chief of an aquarium company. He also worked at two medical technology companies.





















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
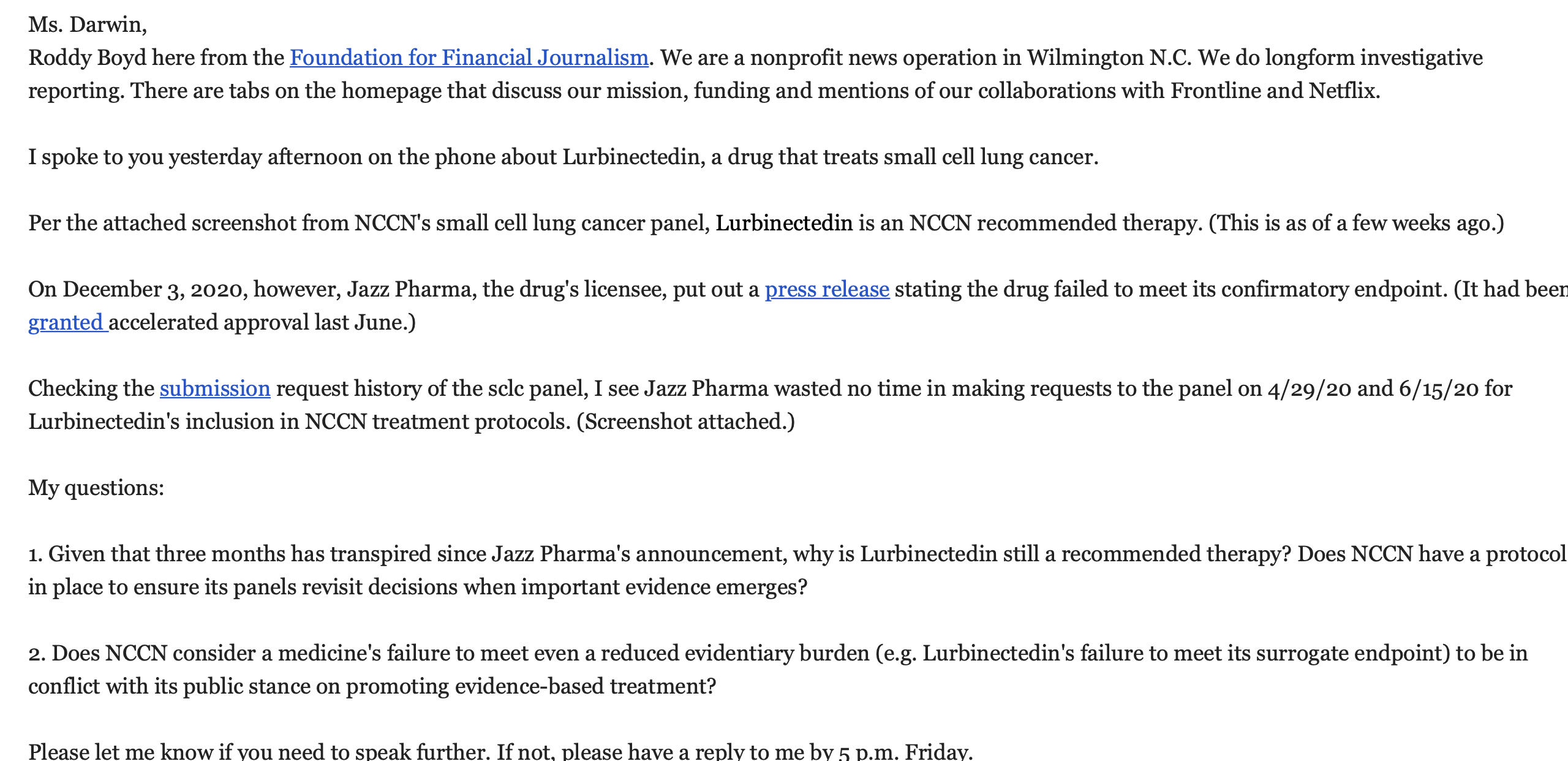{kind=link}
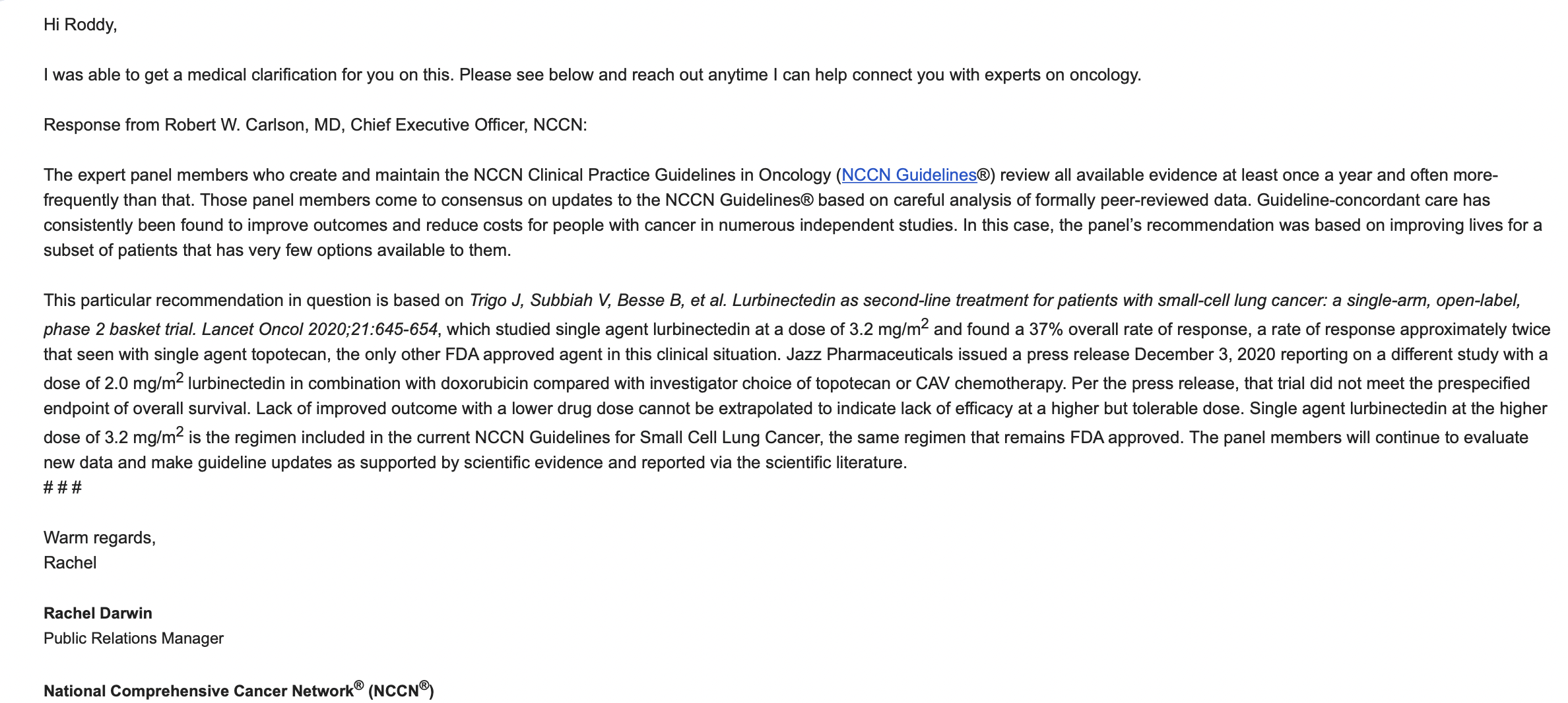{kind=link}
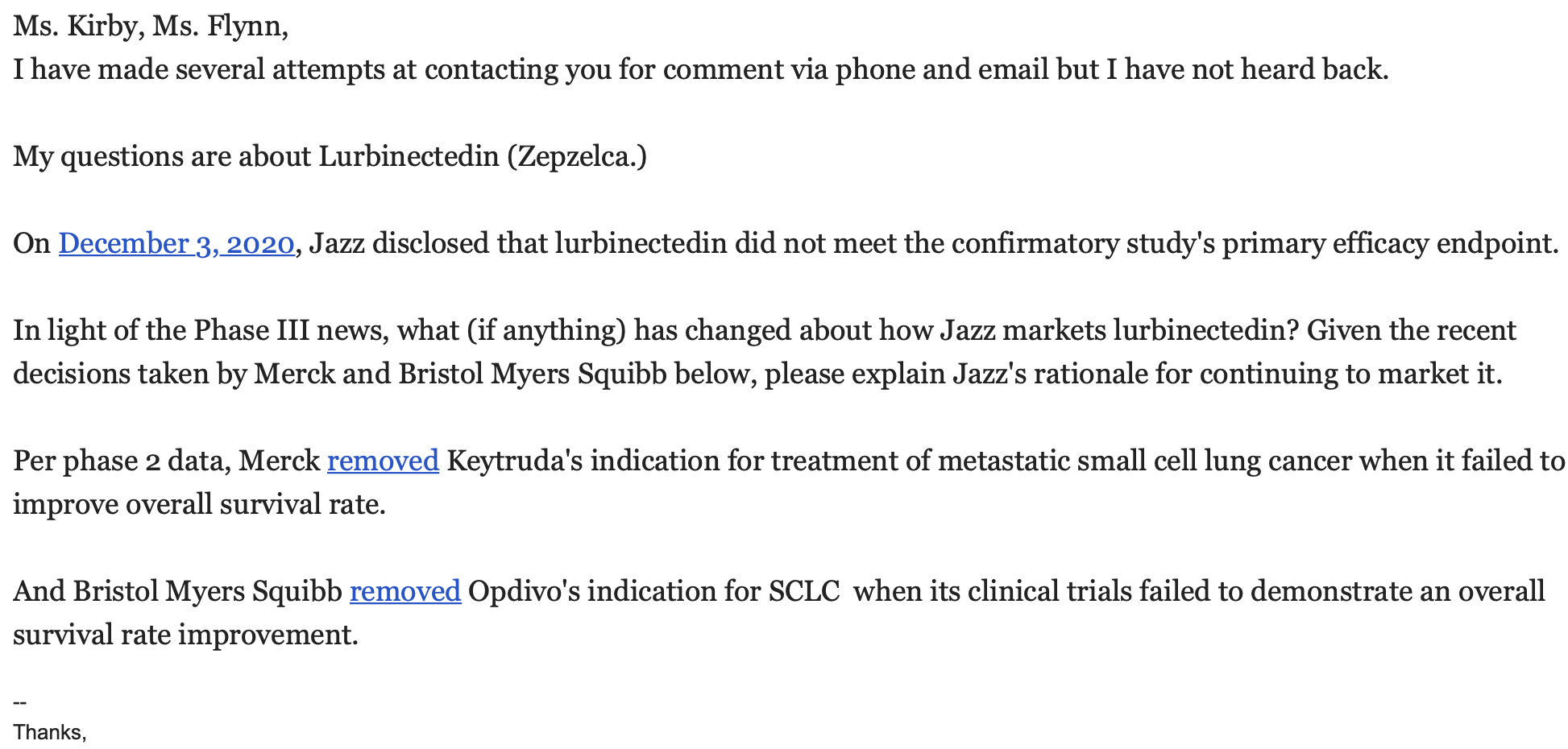{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}