In late June, Jazz Pharmaceuticals began to market a drug aimed at treating people whose metastatic small cell lung cancer has not responded to an initial round of chemotherapy.
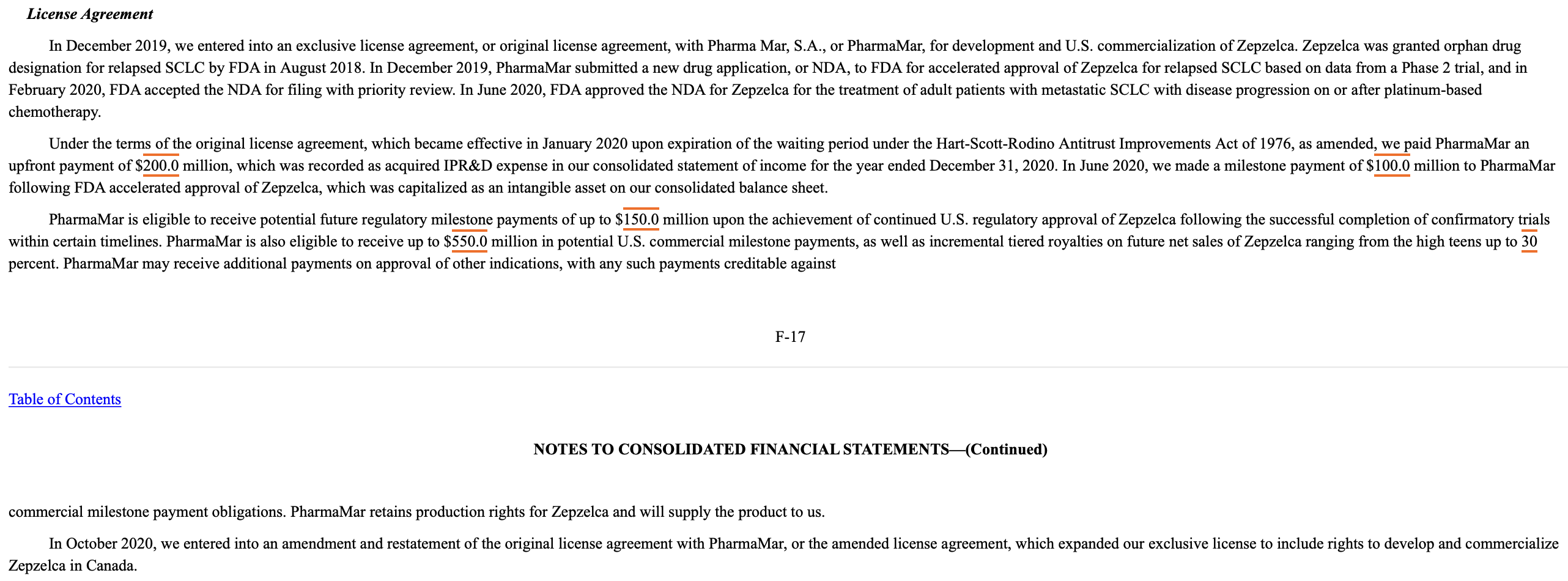
The drug, lurbinectedin, was developed by Madrid-based PharmaMar S.A., which in December 2019 signed a licensing agreement with Jazz. This permitted Jazz to sell the drug in the United States under the brand name Zepzelca. (Lurbinectedin had failed a clinical trial for ovarian cancer in 2018.) Dublin-based Jazz, with its shares listed on the Nasdaq, has significant U.S. operations in Philadelphia and Palo Alto, California.
For U.S. oncologists who treat individuals with small cell lung cancer, lurbinectedin’s arrival was a big deal. Dr. H. Jack West recalled his cautious optimism upon reading of lurbinectedin’s initial clinical trial results last June, especially since few therapies existed for people with small cell lung cancer.
{kind=link}
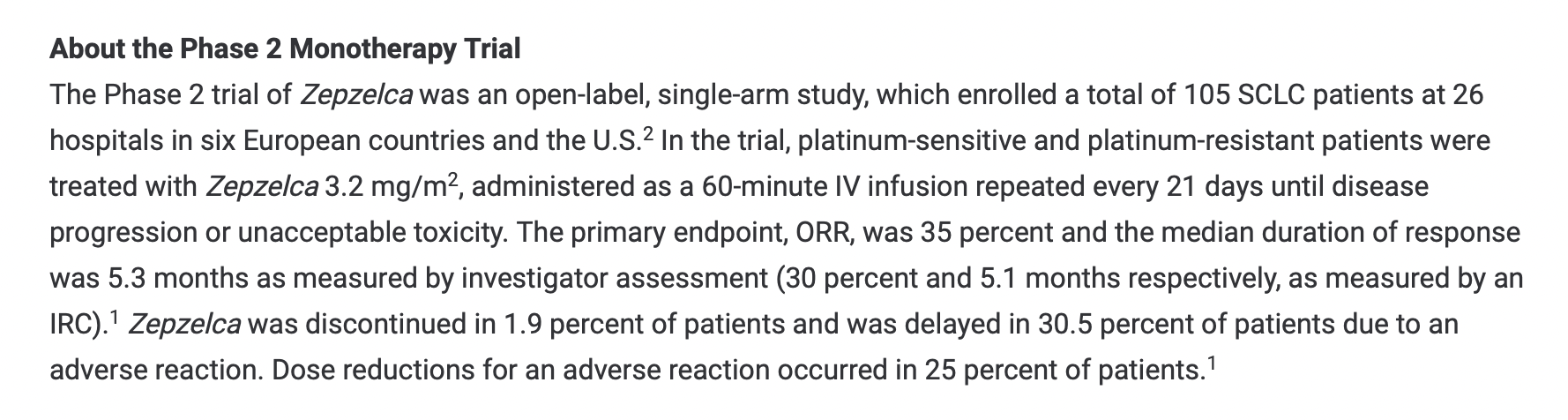
An associate clinical professor in medical oncology at City of Hope’s department of medical oncology and therapeutics research in Duarte, California, West told the Foundation for Financial Journalism that lurbinectedin’s “results in Phase II were [notable] because it was a decent-sized trial [of 105 people] and the drug seemed to have a measurable effect on a subset of patients.”
The meager number of small cell cancer drugs in the development pipeline has led some oncologists to desperately embrace any treatment showing even modest promise, said West, who added that he has seen doctors “cheerleading” for pharmaceutical companies with products in trials and forgoing skepticism about existing treatments.
Despite the fact that Zepzelca was on the market for only six months of last year, it generated 4 percent of Jazz’s 2020 revenue, or $90.4 million. Jazz’s investors apparently loved the earnings boost from lurbinectedin sales; the company’s market capitalization climbed by more than $1.7 billion.
{kind=link}
But the Food and Drug Administration has permitted lurbinectedin’s sale in the United States only under its accelerated approval program. The FDA required that PharmaMar conduct a confirmatory trial to prove the drug’s clinical benefit before seeking full approval.
PharmaMar had initially proposed in December 2018 that Phase III of lurbinectedin’s clinical trial serve as its confirmatory trial; the FDA granted this request in June 2020. (The FDA requests confirmatory trials only for accelerated approval program drugs.)
{kind=link}
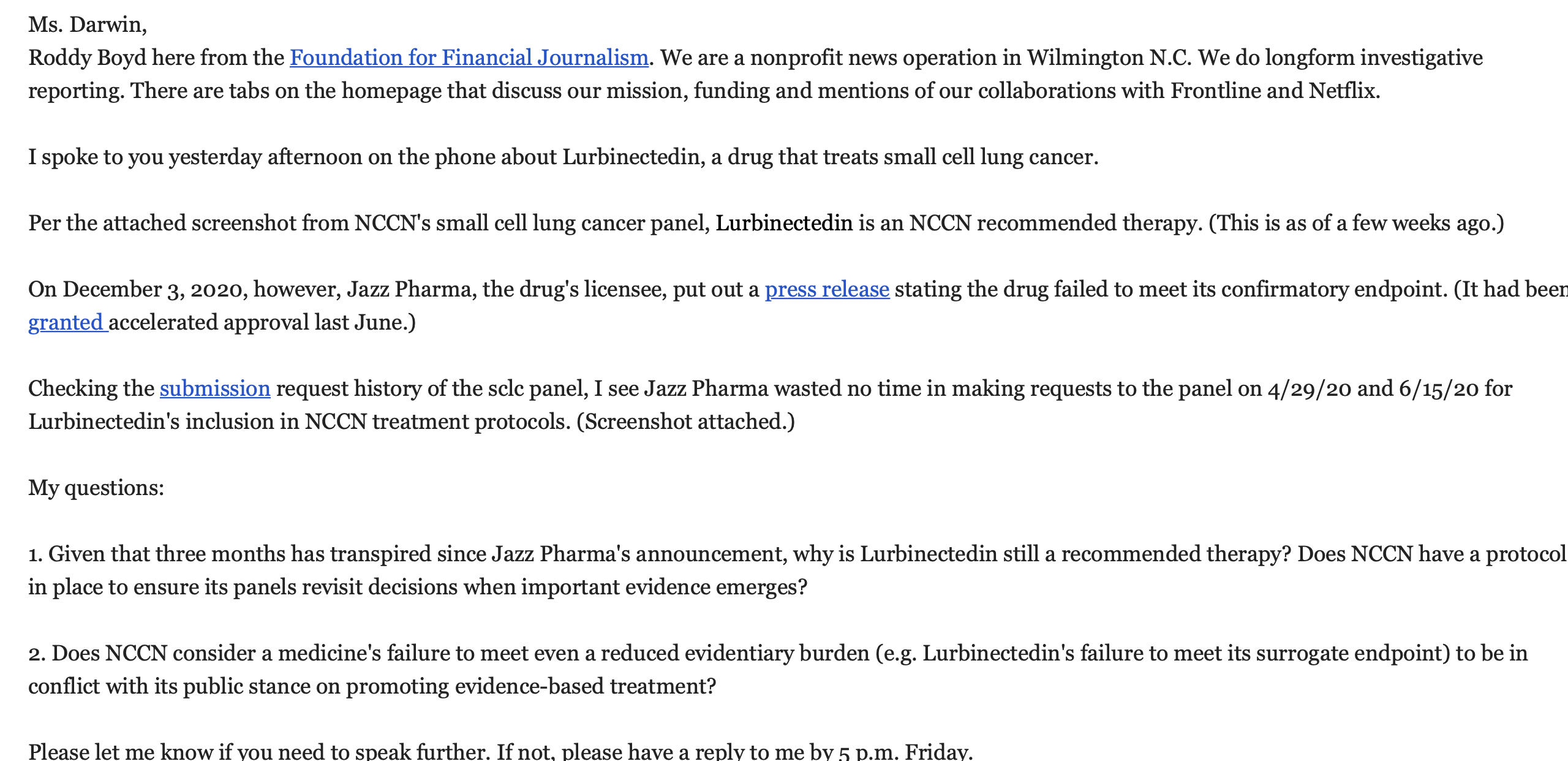
Yet by Dec. 3, Jazz and PharmaMar disclosed that lurbinectedin had failed to meet the primary endpoint of its clinical trial’s Phase III: achieving improvement in the overall survival of participants. The medication did not succeed in proving its benefit to study participants over the standard of care offered by already approved treatments for small cell lung cancer.
The FDA, however, did not pull the drug off the market. This lack of a response is becoming commonplace: The agency has permitted many drugs in the accelerated approval program to remain commercially available after their Phase III clinical trial failures.
Tackling daunting hurdles
While many cancers are lethal, and cancer treatments are generally complex and expensive, small cell lung cancer poses a special challenge.
Named after the cancer cell’s size and shape when viewed through a microscope, small cell lung cancer will cause about 13 percent of the 235,760 newly diagnosed cases of lung cancer in the United States this year, the American Society of Clinical Oncology has projected. Compared with the wealth of information known about other cancers, relatively little is understood about how small cell lung cancer metastasizes. The tumors typically develop in air passages around the windpipe — especially in older smokers — and rapidly spread to other organs. This happens so quickly that almost 70 percent of individuals with the disease have experienced metastasis by the time of their first diagnosis. Chemotherapy might later appear to have eradicated tumors, only to have them grow back.
Just 6 percent of people diagnosed with metastatic small cell lung cancer live five more years, according to the American Society of Clinical Oncology. In comparison, 13 percent of people diagnosed with metastatic pancreatic cancer reach that milestone.
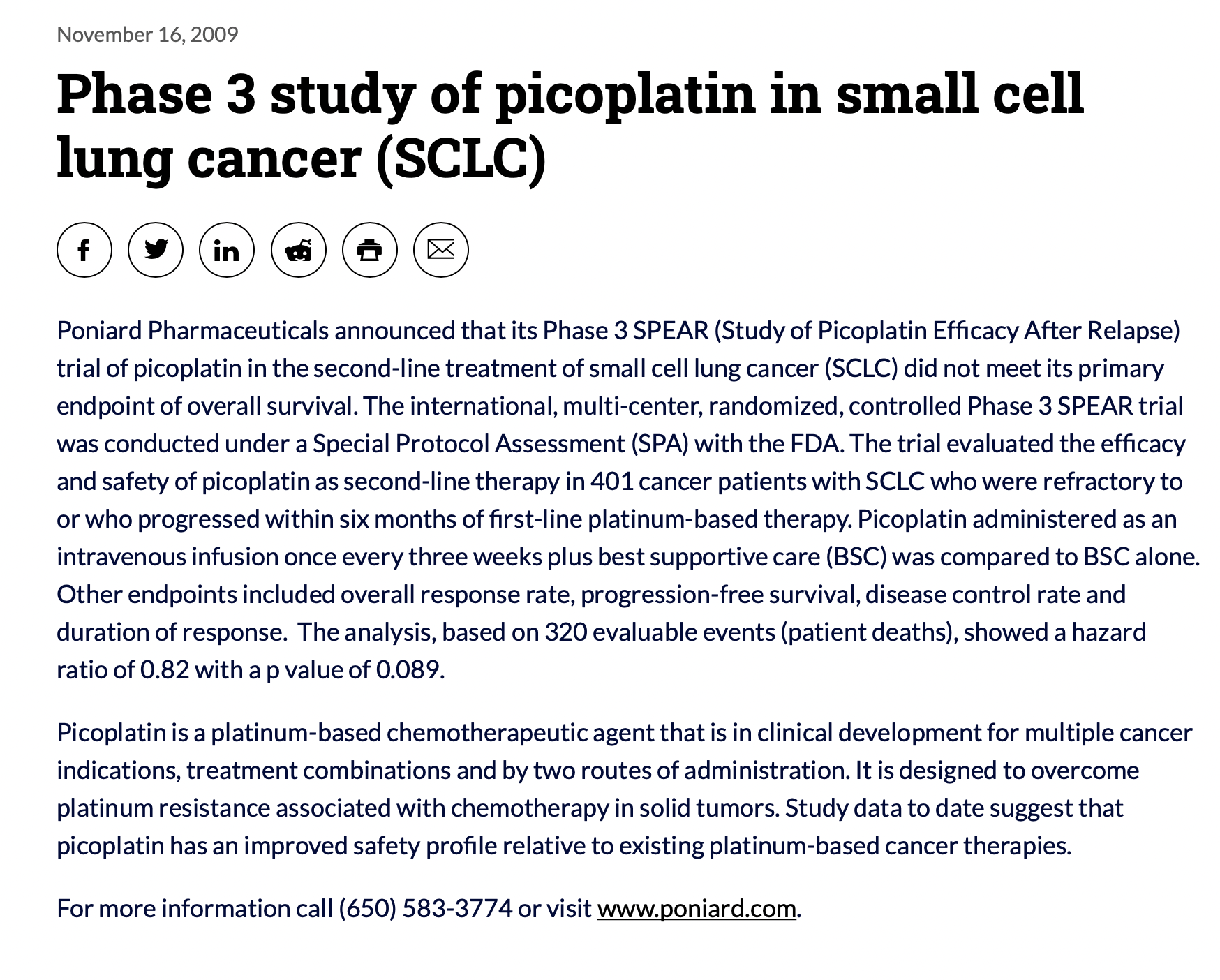
Pharmaceutical companies such as AbbVie, Poniard Pharmaceuticals and United Therapeutics have poured billions of dollars into the development of drugs for small cell lung cancer and clinical trials, but few life-extending options have materialized over the past three decades. All told, 40 clinical trials for small cell lung cancer treatments have failed.
{kind=link}
Failing scientifically, yet scoring commercially
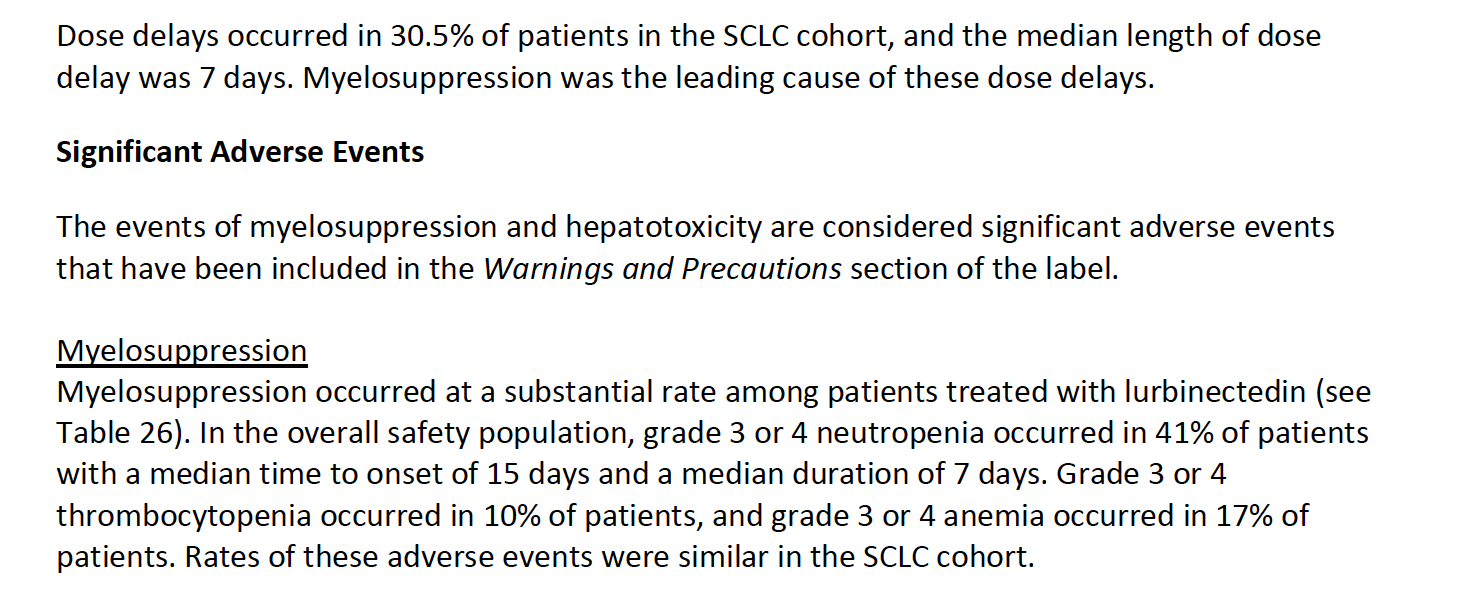
Traditionally, the FDA has viewed a drug’s inability to outperform current treatments in extending or improving the life of study participants as disqualifying — except for medications in its accelerated approval program, such as lurbinectedin. And lurbinectedin, like many cancer drugs, has documented side effects including fatigue, nausea and declines in white blood cell counts.
{kind=link}
Commercially, though, lurbinectedin has been far from a failure, and brokerage analysts have projected that Jazz could take in $200 million to $225 million in revenue this year from sales of the drug. One Wells Fargo analyst, in a June 2020 research note went so far as to suggest that Zepzelca’s annual sales might peak at $700 million. PharmaMar is benefitting handsomely, too: Jazz’s annual report noted the $300 million in payments it made to PharmaMar last year.
{kind=link}
{kind=link}
And the actions of Jazz stand in sharp contrast with those of larger rivals with oncology drugs. After Bristol Myers Squibb and Merck recently disclosed the failure of confirmatory trials for their own bestselling drugs under accelerated FDA approval for treatment of small cell lung cancer, both companies immediately stopped marketing them for that purpose and removed the indication from their labels. Bristol Myers Squibb’s Opdivo and Merck’s Keytruda are still indicated for the treatment of other cancers, including non-small cell lung cancer, though.
{kind=link}
The FDA is rather vague about what is supposed to happen after a drug in the accelerated approval program fails its confirmatory trial. The FDA’s website simply states that the agency has “procedures in place that could lead to removing the drug from market.”
{kind=link}
FDA press officer Chanapa Tantibanchachai wrote in an email reply to the Foundation for Financial Journalism’s questions, “The FDA is committed to ensuring the integrity of the accelerated approval program. The agency is currently in the process of evaluating oncology accelerated approvals.”
{kind=link}
{kind=link}
(On April 27, the FDA’s Oncologic Drugs Advisory Committee will hold a public hearing to examine accelerated approval drugs “with confirmatory trials that have not verified clinical benefits,” the agency has announced.)
{kind=link}
Over the past two decades, the FDA appears to have shifted away from evaluating a drug solely on its trial data in favor of also including other data sets, according to Dr. Thomas Frieden, a former director of the Centers for Disease Control and Prevention. Thus, U.S. regulators might not remove medications like lurbinectedin from the marketplace in the near future.
At the center of this shifting regulatory landscape is the FDA’s acting leader, Dr. Janet Woodcock, who has served two long stints at the helm of the agency’s Center for Drug Evaluation and Research. Dr. Woodcock has been a vocal advocate of accommodating the pharmaceutical industry to speed the availability of drugs. She is well-known for regulatory leniency toward drugs whose clinical trials cast doubts on their efficacy.
What is less clear is how people with small cell lung cancer would benefit from access to expensive drugs that rarely work well, if at all.
Sacrificing clinical rigor, a casualty of war on cancer
The nature of cancer, and particularly small cell lung cancer, results in very complex and brutal tradeoffs as researchers and pharmaceutical companies hasten to bring new drugs to market.
While the randomized controlled trial has been long accepted as the best way to determine whether a drug is effective and safe for the largest possible population, this method poses problems for small cell lung cancer studies.
A clinical trial’s Phase III — which can take as long as four years to assess a drug’s safety and efficacy against the current standard of care — would appear unwieldy if a disease is causing more than 90 percent of the afflicted individuals to die before five years have elapsed.
One technique developed by clinical researchers is using surrogate endpoints, or substitute evaluation criteria. Researchers believe these data points might correlate with two traditional clinical endpoints: extending life or improving its quality.
For example, the data that initially caught Dr. West’s eye in Phase II of lurbinectedin’s clinical trial was a surrogate endpoint called the overall response rate. (The FDA has at times called it an objective response rate.) This can involve measuring a tumor’s size over a period of weeks as a someone takes a drug. (In lurbinectedin’s case, 35 percent of the study participants, or 37 individuals, had their tumors shrink 30 percent or more, with the effect lasting on average slightly less than five months.)
{kind=link}
{kind=link}
Another popular surrogate measurement for cancer trials is progression-free survival. This is calculated from the time after tumors stop growing (or disappear) until they grow again.
While progression-free survival and tumor shrinkage are certainly welcome developments, for people with small cell lung cancer they are often temporary events, given how common it is for tumors to grow back.
What’s more, a 2018 report in Clinical Cancer Research found that overall response rate and progression-free survival are poor predictors of a person’s overall survival.
A more detailed analysis of the tenuous links between response rate and increased patient life appeared in a Journal of the American Medical Association article in May 2019 by three doctors at Oregon Health & Science University: Emerson Chen, Vikram Raghunathan and Vinay Prasad. They examined 85 indications for 59 oncology drugs that were granted FDA approval based on response rate and found that only six of them extended life span. (Some of these drugs were in the accelerated approval program; others were not.)
The FDA does not seem to have taken this research into account, however. In June 2018, FDA researchers published a triumphant review of the accelerated approval program’s first 25 years. From 1992 to 2018, the agency approved 93 indications for 64 products through the program, with only five indications subsequently withdrawn.
But to Harvard Medical School’s Dr. Aaron Kesselheim, the FDA is evaluating its accelerated approval program backward. In a May 2019 JAMA article that made a big splash, Dr. Kesselheim and two colleagues, Drs. Bishal Gyawali and Spencer Phillips Hey, examined the 93 drug indications allowed through the FDA’s accelerated approval program. “We looked ‘underneath the hood’ at the FDA’s basis for approving those [93 indications of] drugs,” said Dr. Kesselheim during a Foundation for Financial Journalism interview. “Our question was simple: ‘Is there evidence that using [the FDA’s accelerated approval] pathway provides drugs that benefit patients?’”
Their answer: not really. Only 19 of the 93 indications investigated by Dr. Kesselheim and his colleagues, or slightly more than 20 percent, demonstrated any improvement in overall survival during Phase III of their clinical trials.
The real problem with the program, said Dr. Kesselheim, lies with the FDA’s use of “surrogate measures that are not clinically validated” for evaluating drugs. “There are valid uses for surrogate endpoints” in clinical trials, he noted: A drug’s effect can be measured faster by using a surrogate endpoint in lieu of a traditional clinical endpoint (which could require two years of study or more.)
“But with no clinical validation, surrogate measures can waste a lot of time,” Dr. Kesselheim added.
Setting standards, while benefitting financially
Another factor in lurbinectedin’s success thus far is tied to the role of the nonprofit National Comprehensive Cancer Network. While most Americans might be unaware of this organization, its work has possibly touched them in some way. As an alliance of 31 cancer treatment hospitals, the network has stated its mission is to develop “evidence-based guidelines” for the screening and treatment of 59 different types of cancer.
{kind=link}
Although adoption of the network’s guidelines is voluntary, health care providers broadly accept its opinions for setting the standard of care for these cancer types. The network’s appeal lies in the fact that its 60 panels of experts include not only experienced oncologists but also pharmacists, research scientists and nurses. The panels investigate the minutiae of treatment details and even make their own assessments of various medicines and dosage levels.
Nonetheless, what health care professionals may not clearly see is how responsive to corporate interests the network’s small cell lung cancer panel has been.
On April 29, Francois Di Trapani, Jazz’s vice president for global scientific affairs, wrote the National Comprehensive Cancer Network’s small cell lung cancer panel to request that its clinical guidelines include lurbinectedin as a treatment option. He then followed up on June 15 to alert the panel to lurbinectedin’s selection for the accelerated access program.
By July 7, the nonprofit network’s small cell lung cancer panel had added lurbinectedin to its clinical practice guidelines.
Yet six doctors among the 30 physicians on this small cell lung cancer panel have disclosed that they have received payment from Jazz: five for serving as a Jazz scientific advisory board member, consultant or expert witness, and one other for participating as a Jazz promotional advisory board or speakers’ bureau member or consultant.
Because the Centers for Medicare and Medicaid Services will not update its Open Payments database of corporate payments to physicians to reflect 2020’s totals until sometime this June, the amounts are not yet publicly available.
One of the network’s six small cell lung cancer panelists who received a Jazz payment gave an enthusiastic November interview to a trade publication, touting lurbinectedin’s prospects: Dr. Apar Ganti, an oncologist and hematologist at the University of Nebraska Medical Center, declared to the American Journal of Managed Care that his panel had swiftly acted to recommend lurbinectedin’s use since few drugs are available to treat small cell lung cancer. His interview did not disclose his acceptance of money from Jazz, the very company marketing the drug in the States.
The Foundation for Financial Journalism reached out for comment to Dr. Ganti and the five other physician panelists paid by Jazz, Drs. Anne Chiang, Afshin Dowlati, Jonathan Goldman, Wade Iams and Jacob Sands but did not hear back.
Asked for comment, the network’s CEO, Dr. Robert Carlson, said the panel chose to recommend lurbinectedin’s use in its clinical guidelines based on a Lancet Oncology study published in May. Carlson added that the panel members make guideline updates “as supported by scientific evidence.” Nonetheless, the Lancet study was funded by PharmaMar and one of its authors, Dr. Sands, is among the six physician panelists who received money from Jazz.
{kind=link}
{kind=link}
Multiple attempts to obtain comment from Jazz’s management were unsuccessful.
{kind=link}